

Lumbar Spine Bone Mineral Apparent Density in Children: Results From the Bone Mineral Density in Childhood Study
- PMID: 30265344
- PMCID: PMC6397436
- DOI: 10.1210/jc.2018-01693
Lumbar Spine Bone Mineral Apparent Density in Children: Results From the Bone Mineral Density in Childhood Study
Abstract
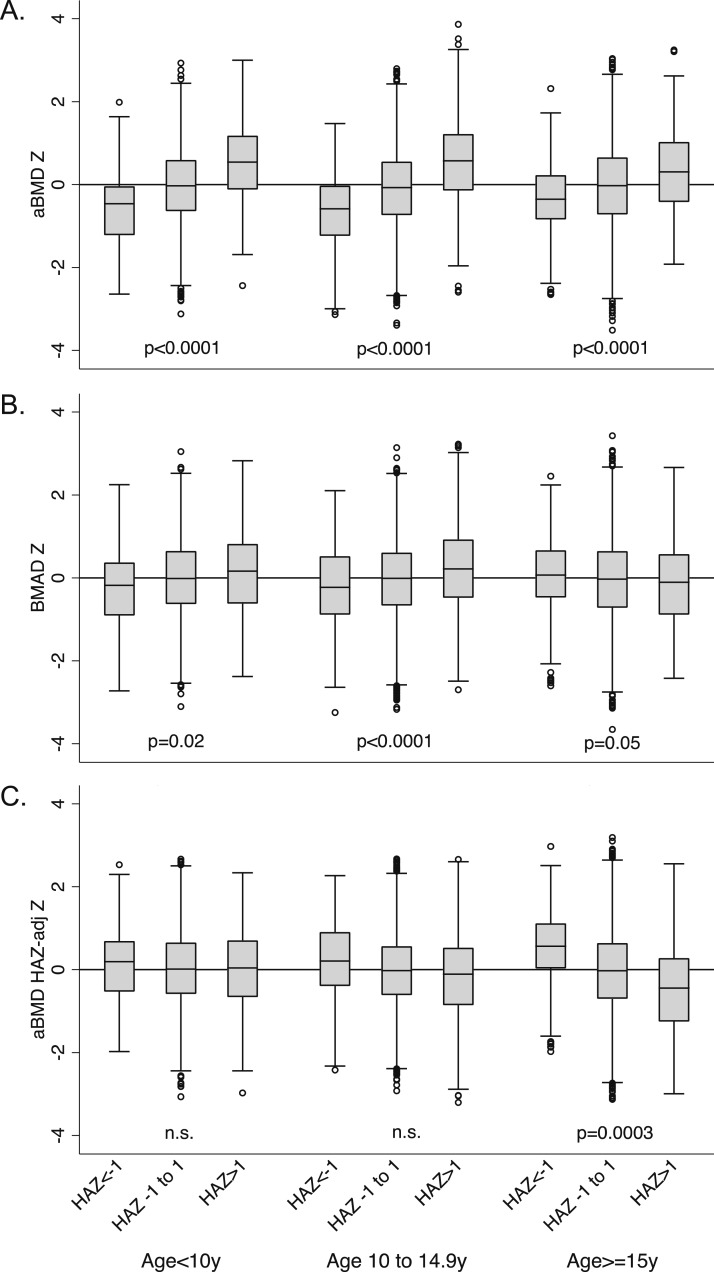
Context: Dual-energy X-ray absorptiometry (DXA) is a cornerstone of pediatric bone health assessment, yet differences in height-for-age confound the interpretation of areal bone mineral density (aBMD) measures. To reduce the confounding of short stature on spine bone density, use of bone mineral apparent density (BMAD) and height-for-age Z-score (HAZ)‒adjusted aBMD (aBMDHAZ) are recommended. However, spine BMAD reference data are sparse, and the degree to which BMAD and aBMDHAZ account for height-related artifacts in bone density remains unclear.
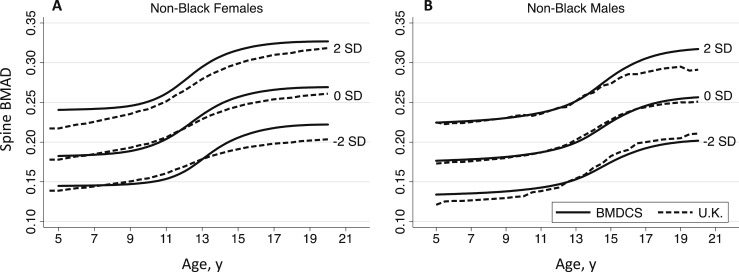
Objective: We developed age-, sex-, and population ancestry‒specific spine BMAD reference ranges; compared height-adjustment methods in accounting for shorter stature; and assessed the stability of these measures over time.
Design: Secondary analysis of data from a previous longitudinal study.
Participants: Children and adolescents aged 5 to 19 years at baseline (n = 2014; 922 males; 22% black) from the Bone Mineral Density in Childhood Study.
Main outcome measures: Lumbar spine BMAD and aBMDHAZ from DXA.
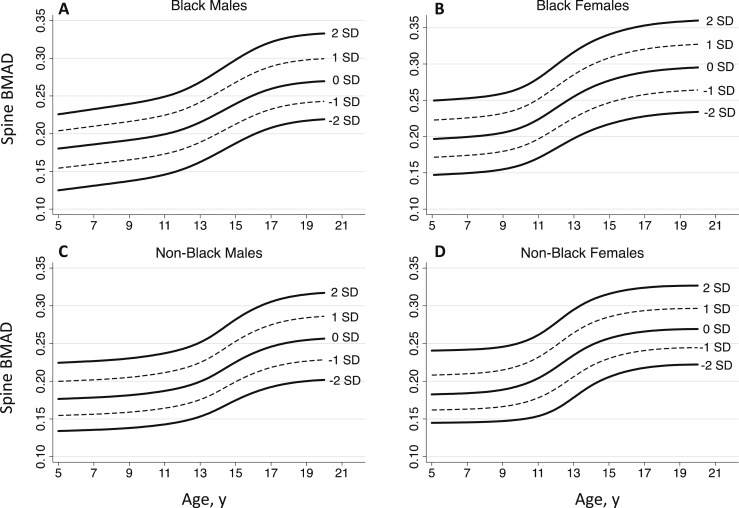
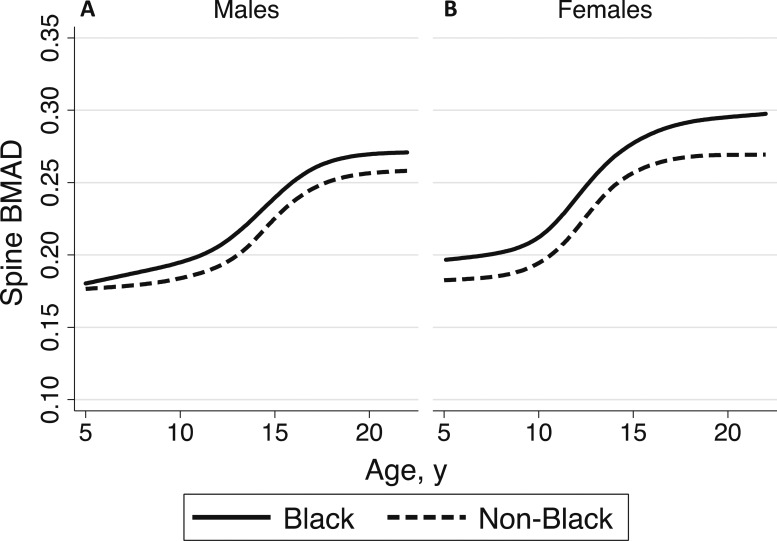
Results: Spine BMAD increased nonlinearly with age and was greater in blacks and females (all P < 0.001). Age-specific spine BMAD z-score reference curves were constructed for black and non‒black males and females. Overall, both BMAD and aBMDHAZz scores reduced the confounding influence of shorter stature, but neither was consistently unbiased across all age ranges. Both BMAD and aBMDHAZz scores tracked strongly over 6 years (r = 0.70 to 0.80; all P < 0.001).
Conclusion: This study provided robust spine BMAD reference ranges and demonstrated that BMAD and aBMDHAZ partially reduced the confounding influence of shorter stature on bone density.
Copyright © 2019 Endocrine Society.
Figures
References
-
- Bachrach LK, Gordon CM, Section on Endocrinology . Bone densitometry in children and adolescents. Pediatrics. 2016;138(4):e20162398. - PubMed
-
- Zemel BS, Leonard MB, Kelly A, Lappe JM, Gilsanz V, Oberfield S, Mahboubi S, Shepherd JA, Hangartner TN, Frederick MM, Winer KK, Kalkwarf HJ. Height adjustment in assessing dual energy x-ray absorptiometry measurements of bone mass and density in children. J Clin Endocrinol Metab. 2010;95(3):1265–1273. - PMC - PubMed
-
- Kalkwarf HJ, Zemel BS, Gilsanz V, Lappe JM, Horlick M, Oberfield S, Mahboubi S, Fan B, Frederick MM, Winer K, Shepherd JA. The bone mineral density in childhood study: bone mineral content and density according to age, sex, and race. J Clin Endocrinol Metab. 2007;92(6):2087–2099. - PubMed
-
- Weaver CM, Gordon CM, Janz KF, Kalkwarf HJ, Lappe JM, Lewis R, O’Karma M, Wallace TC, Zemel BS. The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: a systematic review and implementation recommendations. Osteoporos Int. 2016;27(4):1281–1386. - PMC - PubMed
-
- Zemel BS, Kalkwarf HJ, Gilsanz V, Lappe JM, Oberfield S, Shepherd JA, Frederick MM, Huang X, Lu M, Mahboubi S, Hangartner T, Winer KK. Revised reference curves for bone mineral content and areal bone mineral density according to age and sex for black and non-black children: results of the bone mineral density in childhood study. J Clin Endocrinol Metab. 2011;96(10):3160–3169. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
