

Impact of catheter-induced iatrogenic coronary artery dissection with or without postprocedural flow impairment: A report from a Japanese multicenter percutaneous coronary intervention registry
- PMID: 30265698
- PMCID: PMC6162084
- DOI: 10.1371/journal.pone.0204333
Impact of catheter-induced iatrogenic coronary artery dissection with or without postprocedural flow impairment: A report from a Japanese multicenter percutaneous coronary intervention registry
Abstract
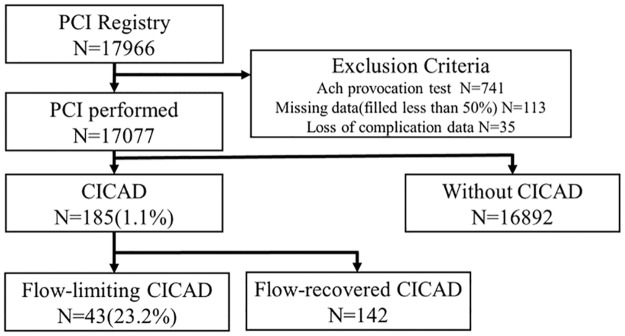
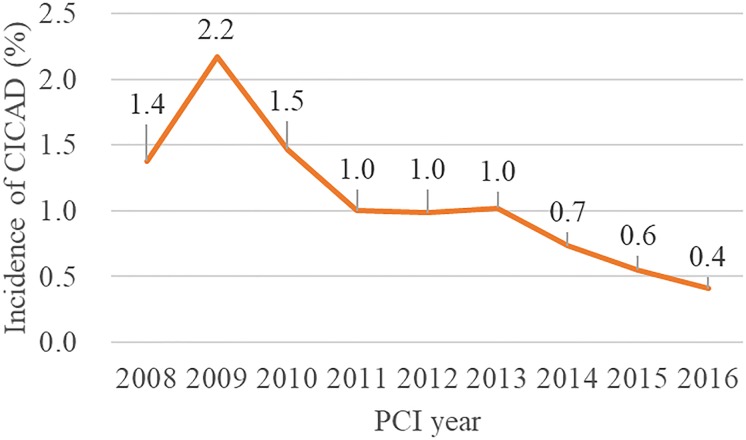
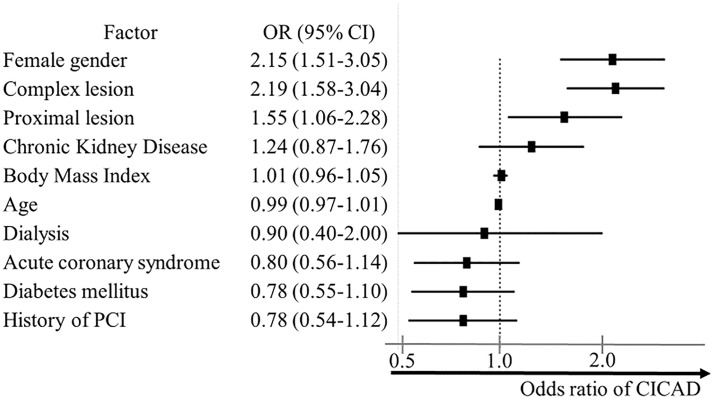
Despite the ever-increasing complexity of percutaneous coronary intervention (PCI), the incidence, predictors, and in-hospital outcomes of catheter-induced coronary artery dissection (CICAD) is not well defined. In addition, there are little data on whether persistent coronary flow impairment after CICAD will affect clinical outcomes. We evaluated 17,225 patients from 15 participating hospitals within the Japanese PCI registry from January 2008 to March 2016. Associations between CICAD and in-hospital adverse cardiovascular events were evaluated using multivariate logistic regression. Outcomes of patients with CICAD with or without postprocedural flow impairment (TIMI flow ≤ 2 or 3, respectively) were analyzed. The population was predominantly male (79.4%; mean age, 68.2 ± 11.0 years); 35.6% underwent PCI for complex lesions (eg. chronic total occlusion or a bifurcation lesion.). CICAD occurred in 185 (1.1%), and its incidence gradually decreased (p < 0.001 for trend); postprocedural flow impairment was observed in 43 (23.2%). Female sex, complex PCI, and target lesion in proximal vessel were independent predictors (odds ratio [OR], 2.18; 95% confidence interval [CI], 1.53-3.10; OR, 2.19; 95% CI, 1.58-3.04; and OR, 1.55; 95% CI, 1.06-2.28, respectively). CICAD was associated with an increased risk of in-hospital adverse events (composite of new-onset cardiogenic shock and new-onset heart failure) regardless of postprocedural flow impairment (OR, 10.9; 95% CI, 5.30-22.6 and OR, 2.27; 95% CI, 1.20-4.27, respectively for flow-impaired and flow-recovered CICAD). In conclusion, CICAD occurred in roughly 1% of PCI cases; female sex, complex PCI, and proximal lesion were its independent risk factors. CICAD was associated with adverse in-hospital cardiovascular events regardless of final flow status. Our data implied that the appropriate selection of PCI was necessary for women with complex lesions.
Conflict of interest statement
The authors have read the journal’s policy and have the following competing interests: Shun Kohsaka received an unrestricted research grant for Department of Cardiology, Keio University School of Medicine from Daiichi-Sankyo Japan. The other authors declare no conflict of interest. This does not alter the authors’ adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Huber MS, Mooney JF, Madison J, Mooney MR. Use of a morphologic classification to predict clinical outcome after dissection from coronary angioplasty. Am J Cardiol. 1991;68(5):467–471. - PubMed
-
- Cappelletti A, Margonato A, Rosano G, Mailhac A, Veglia F, Colombo A, et al. Short- and long-term evolution of unstented nonocclusive coronary dissection after coronary angioplasty. J Am Coll Cardiol. 1999;34(5):1484–1488. - PubMed
-
- Hermans WRM, Rensing BJ, Foley DP, Deckers JW, Rutsch W, Emanuelsson H, et al. Therapeutic dissection after successful coronary balloon angioplasty: No influence on restenosis or on clinical outcome in 693 patients. J Am Coll Cardiol. 1992;20(4):767–780. - PubMed
-
- Venkitachalam L, Kip KE, Selzer F, Wilensky RL, Slater J, Mulukutla SR, et al. Twenty-year evolution of percutaneous coronary intervention and its impact on clinical outcomes—a report from the NHLBI-sponsored, multicenter 1985–86 PTCA and 1997–2006 dynamic registries. Circ Cardiovasc Interv. 2009;2(1):6–13. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
