

Genome-Informed Targeted Therapy for Osteosarcoma
- PMID: 30266815
- PMCID: PMC7134333
- DOI: 10.1158/2159-8290.CD-17-1152
Genome-Informed Targeted Therapy for Osteosarcoma
Abstract
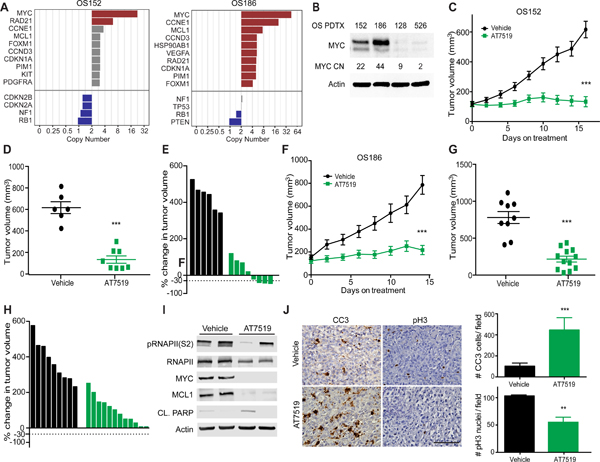
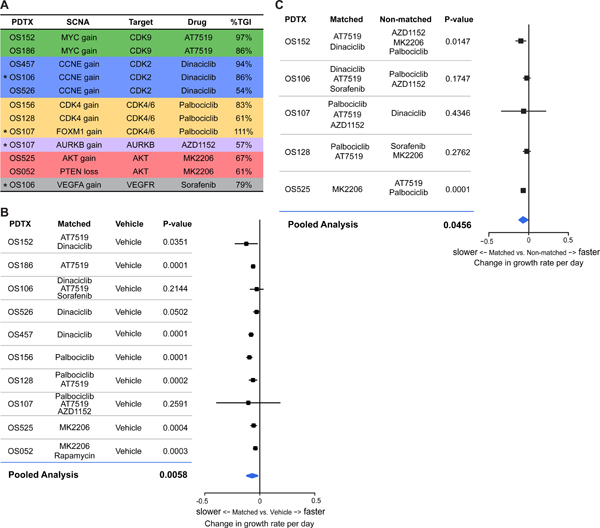
Osteosarcoma is a highly aggressive cancer for which treatment has remained essentially unchanged for more than 30 years. Osteosarcoma is characterized by widespread and recurrent somatic copy-number alterations (SCNA) and structural rearrangements. In contrast, few recurrent point mutations in protein-coding genes have been identified, suggesting that genes within SCNAs are key oncogenic drivers in this disease. SCNAs and structural rearrangements are highly heterogeneous across osteosarcoma cases, suggesting the need for a genome-informed approach to targeted therapy. To identify patient-specific candidate drivers, we used a simple heuristic based on degree and rank order of copy-number amplification (identified by whole-genome sequencing) and changes in gene expression as identified by RNA sequencing. Using patient-derived tumor xenografts, we demonstrate that targeting of patient-specific SCNAs leads to significant decrease in tumor burden, providing a road map for genome-informed treatment of osteosarcoma. SIGNIFICANCE: Osteosarcoma is treated with a chemotherapy regimen established 30 years ago. Although osteosarcoma is genomically complex, we hypothesized that tumor-specific dependencies could be identified within SCNAs. Using patient-derived tumor xenografts, we found a high degree of response for "genome-matched" therapies, demonstrating the utility of a targeted genome-informed approach.This article is highlighted in the In This Issue feature, p. 1.
©2018 American Association for Cancer Research.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures




References
-
- Marina NM et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): an open-label, international, randomised controlled trial. Lancet Oncol 17, 1396–1408, doi:10.1016/S1470-2045(16)30214-5 (2016). - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
