

Linear growth following complicated severe malnutrition: 1-year follow-up cohort of Kenyan children
- PMID: 30266874
- PMCID: PMC6556974
- DOI: 10.1136/archdischild-2018-315641
Linear growth following complicated severe malnutrition: 1-year follow-up cohort of Kenyan children
Abstract
Background: Stunting is the most common manifestation of childhood undernutrition worldwide. Children presenting with severe acute malnutrition (SAM) are often also severely stunted. We evaluated linear growth and its determinants after medically complicated SAM.
Methods: We performed secondary analysis of clinical trial data (NCT00934492) from HIV-uninfected Kenyan children aged 2-59 months hospitalised with SAM. Outcome was change in height/length-for-age z-score (HAZ) between enrolment and 12 months later. Exposures were demographic, clinical, anthropometric characteristics and illness episodes during follow-up.
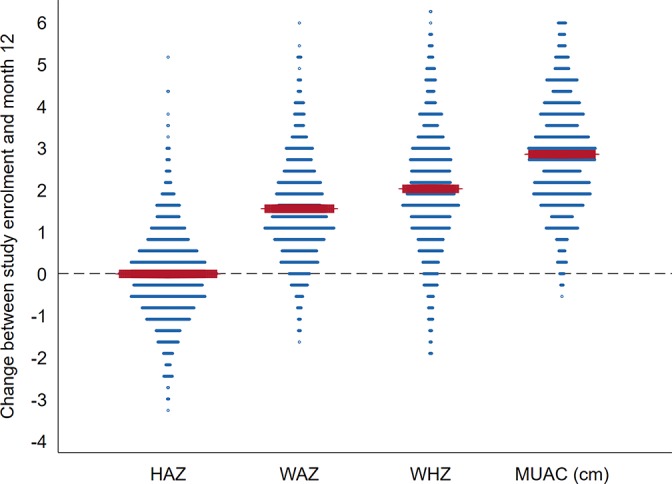
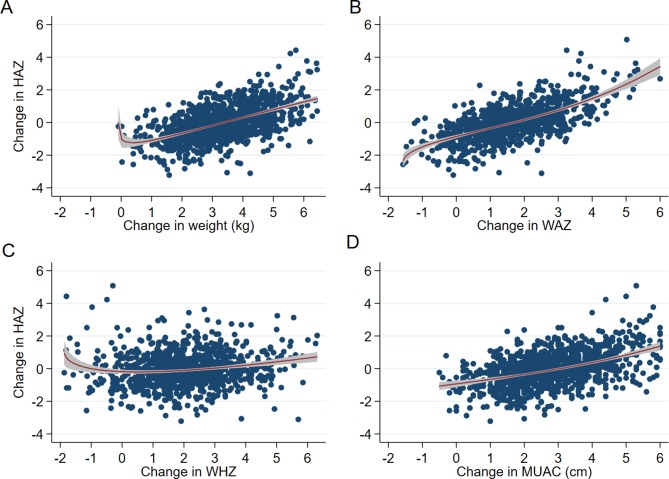
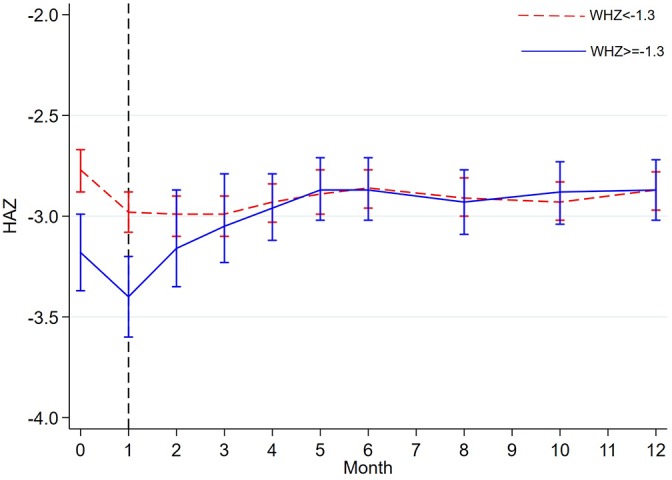
Results: Among 1169 children with HAZ values at month 12 (66% of those in original trial), median (IQR) age 11 (7-17) months and mean (SD) HAZ -2.87 (1.6) at enrolment, there was no change in mean HAZ between enrolment and month 12: -0.006Z (95% CI -0.07 to 0.05Z). While 262 (23%) children experienced minimal HAZ change (within ±0.25 HAZ), 472 (40%) lost >0.25 and 435 (37%) gained >0.25 HAZ. After adjusting for regression to the mean, inpatient or outpatient episodes of diarrhoea and inpatient severe pneumonia during follow-up were associated with HAZ loss. Premature birth and not being cared by the biological parent were associated with HAZ gain. Increases in mid-upper arm circumference and weight-for-age were associated with HAZ gain and protected against HAZ loss. Increase in weight-for-height was not associated with HAZ gain but protected against HAZ loss. No threshold of weight gain preceding linear catch-up growth was observed.
Conclusions: Interventions to improve dietary quality and prevent illness over a longer period may provide opportunities to improve linear growth.
Keywords: growth; height; malnutrition; stunting; undernutrition.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- United Nations Children’s Fund (UNICEF), World Health Organization (WHO), World Bank. Levels and trends in child malnutrition: key findings of the 2018 edition of the joint child malnutrition estimates. New York, Geneva, Washington, DC: UNICEF, WHO, The World Bank, 2018.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical