

Imaging the evolution and pathophysiology of Alzheimer disease
- PMID: 30266970
- PMCID: PMC7032048
- DOI: 10.1038/s41583-018-0067-3
Imaging the evolution and pathophysiology of Alzheimer disease
Abstract
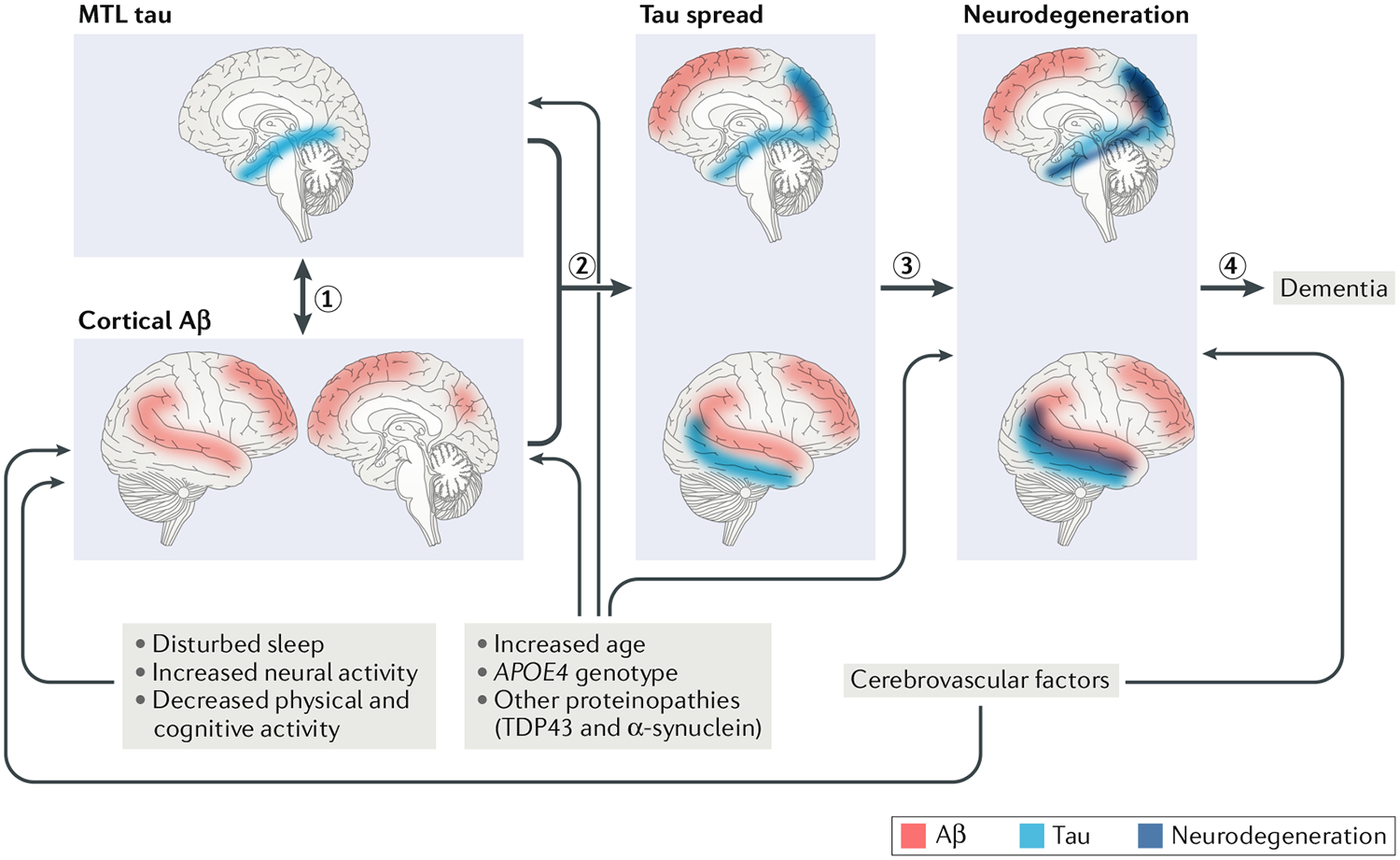
Technologies for imaging the pathophysiology of Alzheimer disease (AD) now permit studies of the relationships between the two major proteins deposited in this disease - amyloid-β (Aβ) and tau - and their effects on measures of neurodegeneration and cognition in humans. Deposition of Aβ in the medial parietal cortex appears to be the first stage in the development of AD, although tau aggregates in the medial temporal lobe (MTL) precede Aβ deposition in cognitively healthy older people. Whether aggregation of tau in the MTL is the first stage in AD or a fairly benign phenomenon that may be transformed and spread in the presence of Aβ is a major unresolved question. Despite a strong link between Aβ and tau, the relationship between Aβ and neurodegeneration is weak; rather, it is tau that is associated with brain atrophy and hypometabolism, which, in turn, are related to cognition. Although there is support for an interaction between Aβ and tau resulting in neurodegeneration that leads to dementia, the unknown nature of this interaction, the strikingly different patterns of brain Aβ and tau deposition and the appearance of neurodegeneration in the absence of Aβ and tau are challenges to this model that ultimately must be explained.
Conflict of interest statement
Competing interests
The author serves as a consultant to BioClinica, Novartis and Genentech.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
