

Carriage of antibiotic-resistant Gram-negative bacteria after discontinuation of selective decontamination of the digestive tract (SDD) or selective oropharyngeal decontamination (SOD)
- PMID: 30268133
- PMCID: PMC6162962
- DOI: 10.1186/s13054-018-2170-2
Carriage of antibiotic-resistant Gram-negative bacteria after discontinuation of selective decontamination of the digestive tract (SDD) or selective oropharyngeal decontamination (SOD)
Abstract
Background: Selective decontamination of the digestive tract (SDD) and selective oropharyngeal decontamination (SOD) reduce colonization with antibiotic-resistant Gram-negative bacteria (ARGNB), incidence of nosocomial infections and improve survival in ICU patients. The effect on bacterial gut colonization might be caused by growth suppression by antibiotics during SDD/SOD. We investigated intestinal colonization with ARGNB after discharge from ICU and discontinuation of SDD or SOD.
Methods: We performed a prospective, observational follow-up study in regular hospital wards of three teaching hospitals in the Netherlands in patients discharged from the ICU, who were participating in a cluster randomized trial comparing SDD with SOD. We determined rectal carriage with ARGNB at ICU discharge (time (T) = 0) and 3, 6 and 10 days after discharge. The primary endpoint was time to first colonization with ARGNB that was not present at T = 0. Bacteria that are intrinsically resistant to antibiotics were not included in the primary analysis, but were included in post-hoc analysis.
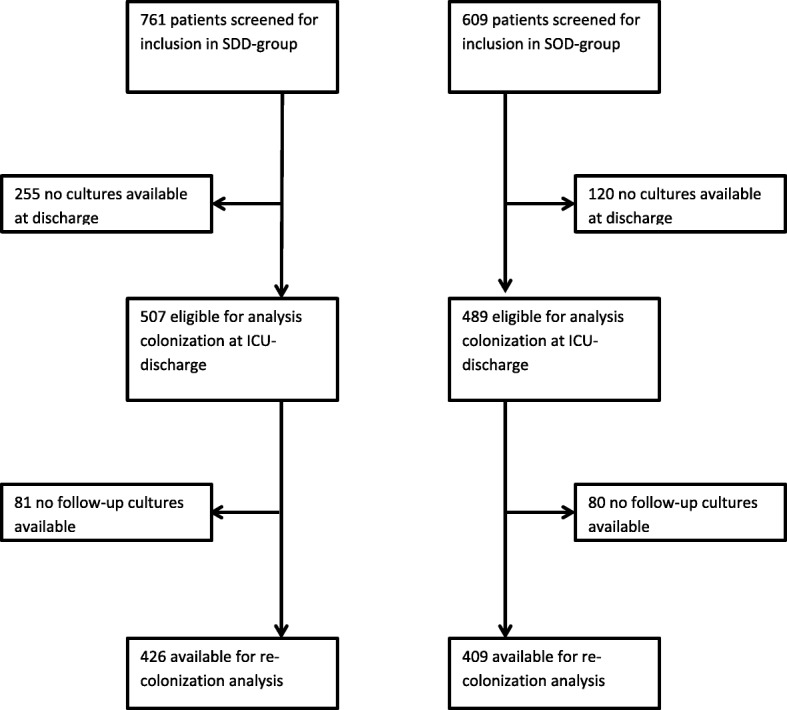
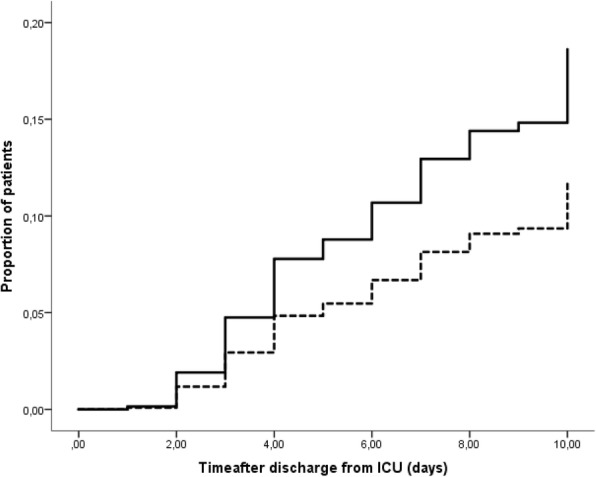
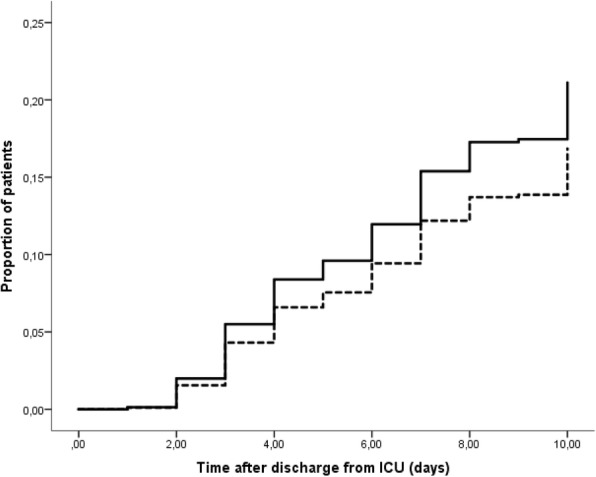
Results: Of 1370 patients screened for inclusion, 996 patients had samples at T = 0 (507 after SDD and 489 after SOD). At ICU discharge, the prevalence of intestinal carriage with any ARGNB was 22/507 (4.3%) after SDD and 87/489 (17.8%) after SOD (p < 0.0001): 426 (SDD) and 409 (SOD) patients had at least one follow-up sample for analysis. The hazard rate for acquiring carriage of ARGNB after discontinuation of SDD, compared to SOD, in the ICU was 0.61 (95% CI 0.40-0.91, p = 0.02), and cumulative risks of acquisition of at least one ARGNB until day 10 were 13% (SDD) and 18% (SOD). At day 10 after ICU discharge, the prevalence of intestinal carriage with ARGNB was 11.3% (26/230 patients) after SDD and 12.5% (28/224 patients) after SOD (p = 0.7). In post-hoc analysis of all ARGNB, including intrinsically resistant bacteria, colonization at ICU discharge was lower after SDD (4.9 vs. 22.3%, p < 0.0001), but acquisition rates after ICU discharge were similar in both groups.
Conclusions: Intestinal carriage at ICU discharge and the acquisition rate of ARGNB after ICU discharge are lower after SDD than after SOD. The prevalence of intestinal carriage with ARGNB at 10 days after ICU discharge was comparable in both groups, suggesting rapid clearance of ARGNB from the gut after ICU discharge.
Trial registration: Netherlands Trial Registry, NTR3311 . Registered on 28 february 2012.
Keywords: Antibiotic resistance; Decolonization; Gram-negative bacteria; Intensive care; Selective digestive tract decontamination; Selective oropharyngeal decontamination.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was granted by the Medical Ethical Committee of the Leiden University Medical Center (CME-V006). The need for informed consent was waived in view of the observational character of the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Plantinga NL, de Smet A, Oostdijk EAN, de Jonge E, Camus C, Krueger WA, Bergmans D, Reitsma JB, Bonten MJM. Selective digestive and oropharyngeal decontamination in medical and surgical ICU patients: individual patient data meta-analysis. Clin Microbiol Infect. 2017;1(17):30477–30479. - PubMed
-
- de Jonge E, Schultz MJ, Spanjaard L, Bossuyt PM, Vroom MB, Dankert J, Kesecioglu J. Effects of selective decontamination of digestive tract on mortality and acquisition of resistant bacteria in intensive care: a randomised controlled trial. Lancet. 2003;362(9389):1011–1016. doi: 10.1016/S0140-6736(1003)14409-14401. - DOI - PubMed
-
- Krueger WA, Lenhart FP, Neeser G, Ruckdeschel G, Schreckhase H, Eissner HJ, Forst H, Eckart J, Peter K, Unertl KE. Influence of combined intravenous and topical antibiotic prophylaxis on the incidence of infections, organ dysfunctions, and mortality in critically ill surgical patients: a prospective, stratified, randomized, double-blind, placebo-controlled clinical trial. Am J Respir Crit Care Med. 2002;166(8):1029–1037. doi: 10.1164/rccm.2105141. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
