

A complete and multifaceted overview of antibiotic use and infection diagnosis in the intensive care unit: results from a prospective four-year registration
- PMID: 30268142
- PMCID: PMC6162888
- DOI: 10.1186/s13054-018-2178-7
A complete and multifaceted overview of antibiotic use and infection diagnosis in the intensive care unit: results from a prospective four-year registration
Abstract
Background: Preparing an antibiotic stewardship program requires detailed information on overall antibiotic use, prescription indication and ecology. However, longitudinal data of this kind are scarce. Computerization of the patient chart has offered the potential to collect complete data of high resolution. To gain insight in our global antibiotic use, we aimed to explore antibiotic prescription in our intensive care unit (ICU) from various angles over a prolonged time period.
Methods: We studied all adult patients admitted to Ghent University Hospital ICU from 1 January 2013 until 31 December 2016. Antibiotic prescription data were prospectively merged with diagnostic (suspected focus, severity and probability of infection at the time of prescription, or prophylaxis) and microbiology data by ICU physicians during daily workflow through dedicated software. Definite focus of infection and probability of infection (classified as high/moderate/low) were reassessed by dedicated ICU physicians at patient discharge.
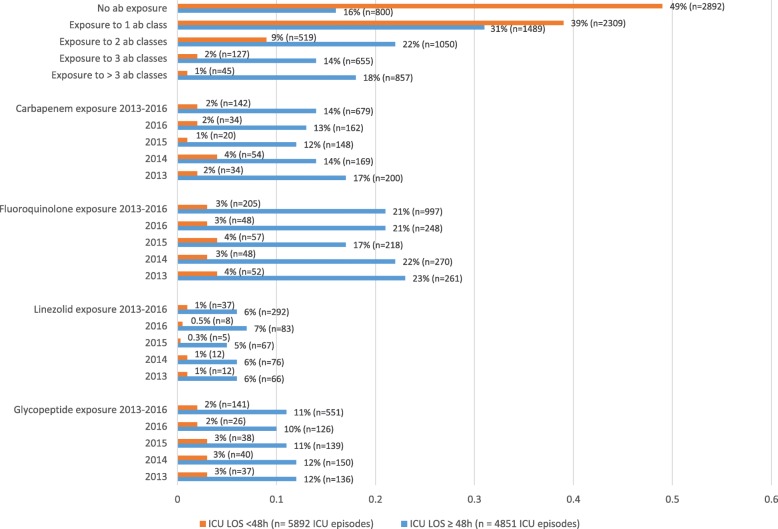
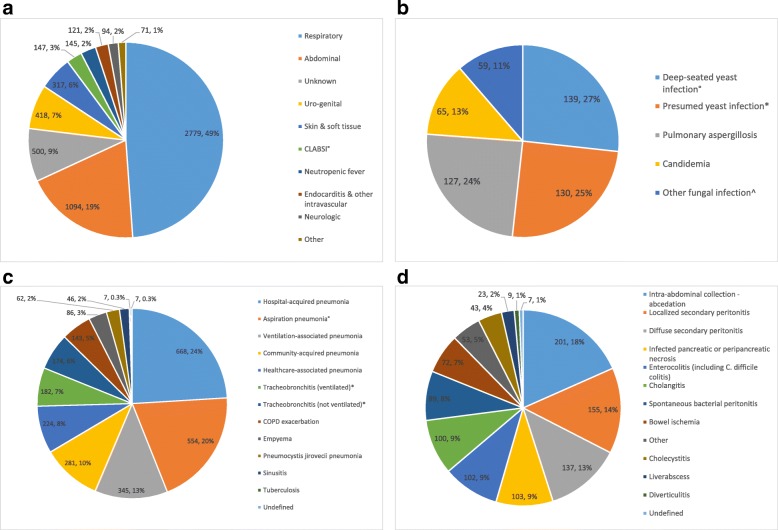
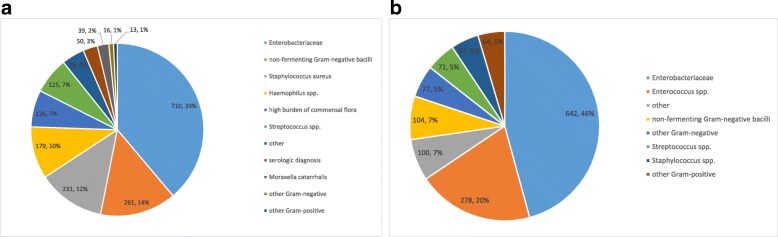
Results: During the study period, 8763 patients were admitted and overall antibiotic consumption amounted to 1232 days of therapy (DOT)/1000 patient days. Antibacterial DOT (84% of total DOT) were linked with infection in 80%; the predominant foci were the respiratory tract (49%) and the abdomen (19%). A microbial cause was identified in 56% (3169/5686). Moderate/low probability infections accounted for 42% of antibacterial DOT prescribed for respiratory tract infections; for abdominal infections, this figure was 15%. The median treatment duration of moderate/low probability respiratory infections was 4 days (IQR 3-7). Antifungal DOT (16% of total DOT) were linked with infection in 47% of total antifungal DOT. Antifungal prophylaxis was primarily administered in the surgical ICU (76%), with a median duration of 4 DOT (IQR 2-9).
Conclusions: By prospectively combining antibiotic, microbiology and clinical data we were able to construct a longitudinal, multifaceted dataset on antibiotic use and infection diagnosis. A complete overview of this kind may allow the identification of antibiotic prescription patterns that require future antibiotic stewardship attention.
Keywords: Antibiotic stewardship; Electronic surveillance; Infection; Intensive care unit; Longitudinal surveillance.
Conflict of interest statement
Ethics approval and consent to participate
The Ghent University Hospital Ethics Committee approved the study (registration number B670201628197) and waived informed consent based on the non-interventional nature of this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, Moreno R, Lipman J, Gomersall C, Sakr Y, Reinhart K, EPIC II group of Investigators International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302:2323–2329. doi: 10.1001/jama.2009.1754. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
