

Refractory out-of-hospital cardiac arrest with ongoing cardiopulmonary resuscitation at hospital arrival - survival and neurological outcome without extracorporeal cardiopulmonary resuscitation
- PMID: 30268147
- PMCID: PMC6162879
- DOI: 10.1186/s13054-018-2176-9
Refractory out-of-hospital cardiac arrest with ongoing cardiopulmonary resuscitation at hospital arrival - survival and neurological outcome without extracorporeal cardiopulmonary resuscitation
Abstract
Background: The prognosis in refractory out-of-hospital cardiac arrest (OHCA) with ongoing cardiopulmonary resuscitation (CPR) at hospital arrival is often considered dismal. The use of extracorporeal cardiopulmonary resuscitation (eCPR) for perfusion enhancement during resuscitation has shown variable results. We aimed to investigate outcome in refractory OHCA patients managed conservatively without use of eCPR.
Methods: We included consecutive OHCA patients with refractory arrest or prehospital return of spontaneous circulation (ROSC) in the Copenhagen area in 2002-2011.
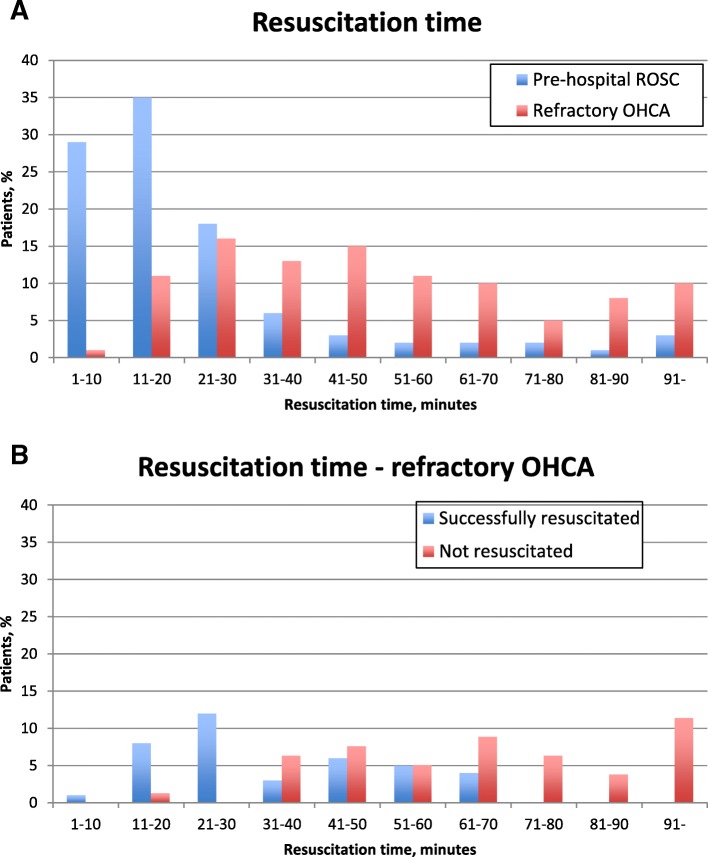
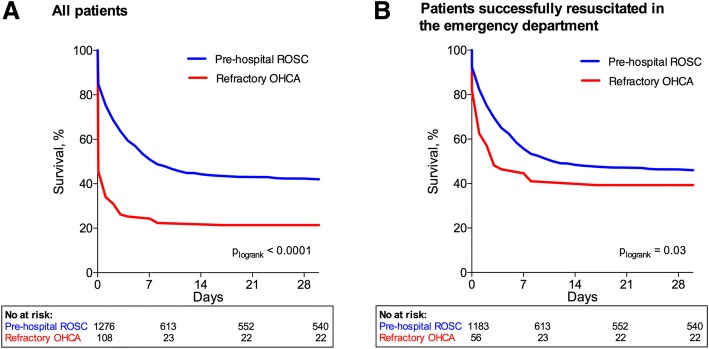
Results: A total of 3992 OHCA patients with resuscitation attempts were included; in 2599, treatment was terminated prehospital, and 1393 (35%) were brought to the hospital either with ROSC (n = 1285, 92%) or with refractory OHCA (n = 108, 8%). Of patients brought in with refractory OHCA, 56 (52%) achieved ROSC in the emergency department. There were no differences between patients with refractory OHCA or prehospital ROSC with regard to age, sex, comorbidities, or etiology of OHCA. Time to emergency medical services (EMS) arrival was similar, whereas time to ROSC (when ROSC was achieved) was longer in refractory OHCA patients (EMS, 6 (5-9] vs. 7 [5-10] min, p = 0.8; ROSC, 15 [9-22] vs. 27 [20-41] min, p < 0.001). Independent factors associated with transport with refractory OHCA instead of prehospital termination of therapy were OHCA in public (OR, 3.6 [95% CI, 2.2-5.8]; p < 0.001), witnessed OHCA (OR, 3.7 [2.0-7.1]; p < 0.001), shockable rhythm (OR, 3.0 [1.9-4.7]; p < 0.001), younger age (OR, 1.2 [1.1-1.2]; p < 0.001), and later calendar year (OR, 1.4 [1.2-1.6]; p < 0.001). Thirty-day survival was 20% in patients with refractory OHCA compared with 42% in patients with prehospital ROSC (p < 0.001). Four of 28 refractory OHCA patients with duration of resuscitation > 60 min achieved ROSC. No difference in favorable neurological outcome in patients surviving to discharge was found (prehospital ROSC 84% vs. refractory OHCA 86%; p = 0.7).
Conclusions: Survival after refractory OHCA with ongoing CPR at hospital arrival was significantly lower than among patients with prehospital ROSC. Despite a lower survival, the majority of survivors with both refractory OHCA and prehospital ROSC were discharged with a similar degree of favorable neurological outcome, indicating that continued efforts in spite of refractory OHCA are not in vain and may still lead to favorable outcome even without eCPR.
Keywords: Cardiac arrest; Ongoing CPR; Refractory cardiac arrest; Survival.
Conflict of interest statement
Ethics approval and consent to participate
The regional ethics committee waived the need for informed consent for the study with the reference number H-2-2012-53, and the study was approved by the Danish Data Protection Agency.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Extracorporeal versus conventional cardiopulmonary resuscitation for refractory out-of-hospital cardiac arrest: a secondary analysis of the Prague OHCA trial.Crit Care. 2022 Oct 27;26(1):330. doi: 10.1186/s13054-022-04199-3. Crit Care. 2022. PMID: 36303227 Free PMC article. Clinical Trial.
-
Relationship between Time-to-ROSC and Survival in Out-of-hospital Cardiac Arrest ECPR Candidates: When is the Best Time to Consider Transport to Hospital?Prehosp Emerg Care. 2016 Sep-Oct;20(5):615-22. doi: 10.3109/10903127.2016.1149652. Epub 2016 Mar 28. Prehosp Emerg Care. 2016. PMID: 27018764
-
Prehospital Advanced Cardiac Life Support for Out-of-hospital Cardiac Arrest: A Cohort Study.Acad Emerg Med. 2017 Sep;24(9):1100-1109. doi: 10.1111/acem.13246. Epub 2017 Aug 16. Acad Emerg Med. 2017. PMID: 28646584
-
Comparing extracorporeal cardiopulmonary resuscitation with conventional cardiopulmonary resuscitation: A meta-analysis.Resuscitation. 2016 Jun;103:106-116. doi: 10.1016/j.resuscitation.2016.01.019. Epub 2016 Feb 2. Resuscitation. 2016. PMID: 26851058 Review.
-
[Venoarterial extracorporeal membrane oxygenation for out-of-hospital cardiac arrest. Case series of prehospital and in-hospital therapies].Anaesthesist. 2015 Aug;64(8):580-5. doi: 10.1007/s00101-015-0058-y. Epub 2015 Jul 21. Anaesthesist. 2015. PMID: 26194653 Review. German.
Cited by
-
Association between Survival and Time of On-Scene Resuscitation in Refractory Out-of-Hospital Cardiac Arrest: A Cross-Sectional Retrospective Study.Int J Environ Res Public Health. 2021 Jan 9;18(2):496. doi: 10.3390/ijerph18020496. Int J Environ Res Public Health. 2021. PMID: 33435406 Free PMC article.
-
Impact of Cardiac Arrest Centers on the Survival of Patients With Nontraumatic Out-of-Hospital Cardiac Arrest: A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2022 Jan 4;11(1):e023806. doi: 10.1161/JAHA.121.023806. Epub 2021 Dec 20. J Am Heart Assoc. 2022. PMID: 34927456 Free PMC article.
-
Expedited transport versus continued on-scene resuscitation for refractory out-of-hospital cardiac arrest: A systematic review and meta-analysis.Resusc Plus. 2023 Oct 7;16:100482. doi: 10.1016/j.resplu.2023.100482. eCollection 2023 Dec. Resusc Plus. 2023. PMID: 37822456 Free PMC article. Review.
-
Potential impacts of a novel integrated extracorporeal-CPR workflow using an interventional radiology and immediate whole-body computed tomography system in the emergency department.BMC Cardiovasc Disord. 2020 Jan 16;20(1):23. doi: 10.1186/s12872-020-01332-4. BMC Cardiovasc Disord. 2020. PMID: 31948395 Free PMC article.
-
Prospective observational study of mechanical cardiopulmonary resuscitation, extracorporeal membrane oxygenation and early reperfusion for refractory cardiac arrest in Sydney: the 2CHEER study.Crit Care Resusc. 2020 Mar;22(1):26-34. doi: 10.51893/2020.1.oa3. Crit Care Resusc. 2020. PMID: 32102640 Free PMC article.
References
-
- Søholm H, Hassager C, Lippert F, Winther-Jensen M, Thomsen JH, Friberg H, et al. Factors associated with successful resuscitation after out-of-hospital cardiac arrest and temporal trends in survival and comorbidity. Ann Emerg Med. 2015;65:523–531.e2. doi: 10.1016/j.annemergmed.2014.12.009. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
