

Cost-effectiveness analysis of lumacaftor and ivacaftor combination for the treatment of patients with cystic fibrosis in the United States
- PMID: 30268148
- PMCID: PMC6162947
- DOI: 10.1186/s13023-018-0914-3
Cost-effectiveness analysis of lumacaftor and ivacaftor combination for the treatment of patients with cystic fibrosis in the United States
Abstract
Background: Lumacaftor/ivacaftor was approved by the Food and Drug Administration (FDA) as a combination treatment for Cystic Fibrosis (CF) patients who are homozygous for the F508del mutation. The objective of this study was to assess the cost-effectiveness of lumacaftor/ivacaftor combination for the treatment of CF homozygous for F508del CF Transmembrane Conductance Regulator (CFTR) mutation.
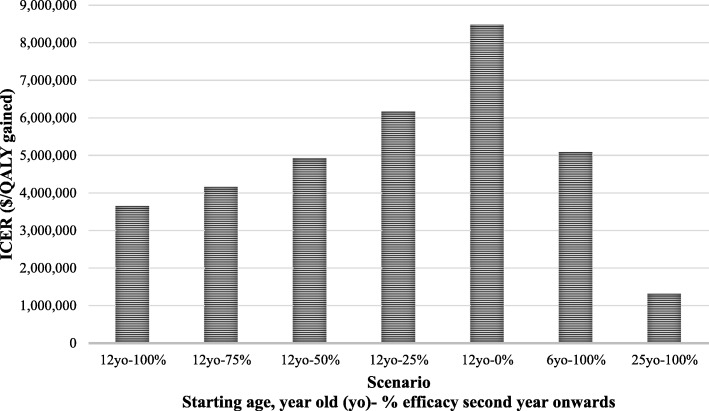
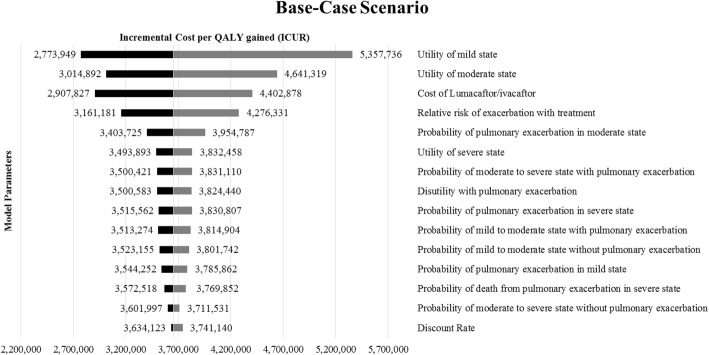
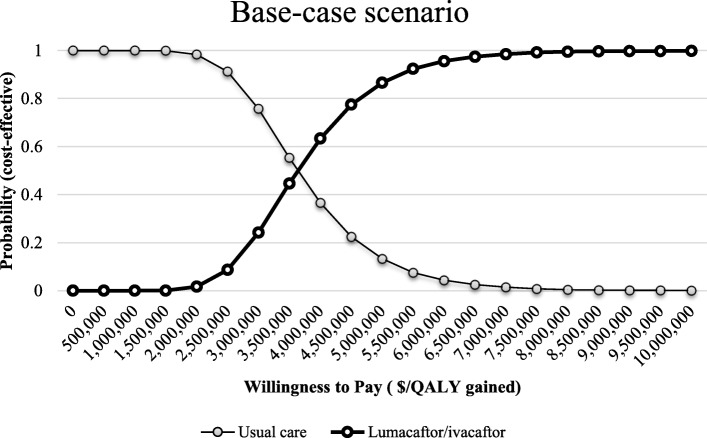
Methods: A Markov-state transition model following a cohort of 12 year-old CF patients homozygous for F508del CFTR mutation in the United States (US) over two, four, six, eight and ten years from a payer's perspective was developed using TreeAge Pro 2016. Markov states included: mild (percentage of predicted forced expiratory volume in 1 s or FEV1 > 70%), moderate (FEV1 40-70%), severe (FEV1 < 40%) disease, post-transplant, and death. Pulmonary exacerbation and lung transplant were included as transition states. All the input parameters were estimated from the literature. A 1-year cycle length and 3% discount rate were applied. To assess uncertainty in long-term treatment effects, several scenarios were modelled: 100% long-term effectiveness (base-case), defined as improvement in FEV1 in the first year followed by no annual FEV1 decline and a constant reduction in pulmonary exacerbations throughout, 75%, 50%, 25% and 0% (worst case) long-term effectiveness, where treatment effects were intermediate from the second year of treatment until the end of the time horizon. Other scenarios included changing the starting age of the cohort to 6 and 25 years. Primary outcome included incremental cost-effectiveness ratio (ICER) in terms of cost per quality adjusted life year (QALY) gained. One-way and probabilistic sensitivity analyses were performed to determine uncertainty.
Results: Under the base-case, Lumacaftor/ivacaftor resulted in higher QALYs (7.29 vs 6.84) but at a very high cost ($1,778,920.88) compared to usual care ($116,155.76) over a 10-year period. The ICER for base-case and worst-case scenarios were $3,655,352 / QALY, and $8,480,265/QALY gained, respectively. In the base-case, lumacaftor/ivacaftor was cost-effective at a threshold of $150,000/QALY-gained when annual drug costs were lower than $4153. The results were not substantially affected by the sensitivity analyses.
Conclusions: The intervention produces large QALY gains but at an extremely high cost, resulting in an ICER that would not typically be covered by any insurer. Lumacaftor/ivacaftor's status as an orphan drug complicates coverage decisions.
Keywords: Cost-effectiveness; Cystic fibrosis; Ivacaftor; Lumacaftor.
Conflict of interest statement
Authors’ information
DRT, PharmD, MA, FCCP, is Full Professor and Takeda Professor in Medication Adherence in the Department of Pharmacy Systems, Outcomes and Policy in the UIC College of Pharmacy. He is an IHRP Fellow and has been a core faculty member of the UIC Center for Pharmacoepidemiology and Pharmacoeconomic Research since August 2005 and an Assistant Director since 2016. He has vast experience of conducting cost-effectiveness analysis for various types of interventions.
MLD, MD, is an Associate Professor of Medicine and Pediatrics and Associate Director, Pediatric Cystic Fibrosis Center at the University of Chicago. She specializes in pulmonary medicine and provides care for adults and children with a range of respiratory disorders, including cystic fibrosis, complex asthma and chronic lung disease.
RNC, MD, MAPP is the Division Chief of Academic Internal Medicine and Geriatrics and Associate Professor of Medicine and a health services researcher at UIC College of medicine. She also holds an affiliate appointment at UIC’s School of Public Health.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- FDA Briefing Document. Pulmonary-allergy drugs advisory Committee meeting. 2015. https://www.fdanews.com/ext/resources/files/05-15/05-11-15-CFbriefing.pd.... Accessed 21 August 2016.
-
- Annual Data Report. Cystic Fibrosis Foundation Patient Registry. 2015. https://www.cff.org/Our-Research/CF-Patient-Registry/2015-Patient-Regist.... Accessed 9 February 2016.
-
- Drugs@FDA: FDA Approved Drug Products. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.... Accessed 17 January 2016.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
