

Development and validation of a radiomics signature for clinically significant portal hypertension in cirrhosis (CHESS1701): a prospective multicenter study
- PMID: 30268833
- PMCID: PMC6197722
- DOI: 10.1016/j.ebiom.2018.09.023
Development and validation of a radiomics signature for clinically significant portal hypertension in cirrhosis (CHESS1701): a prospective multicenter study
Abstract
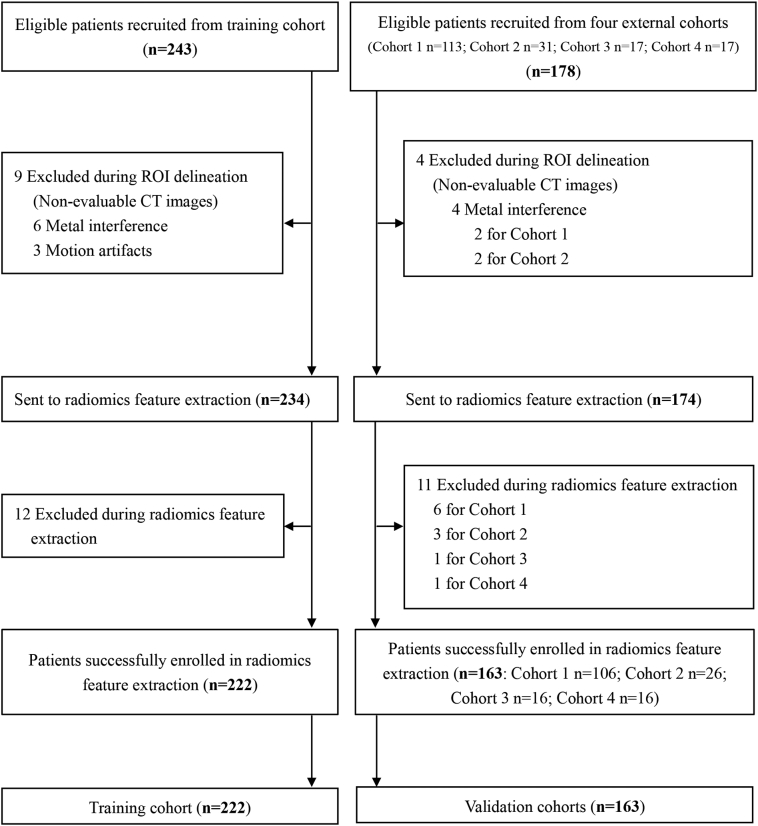
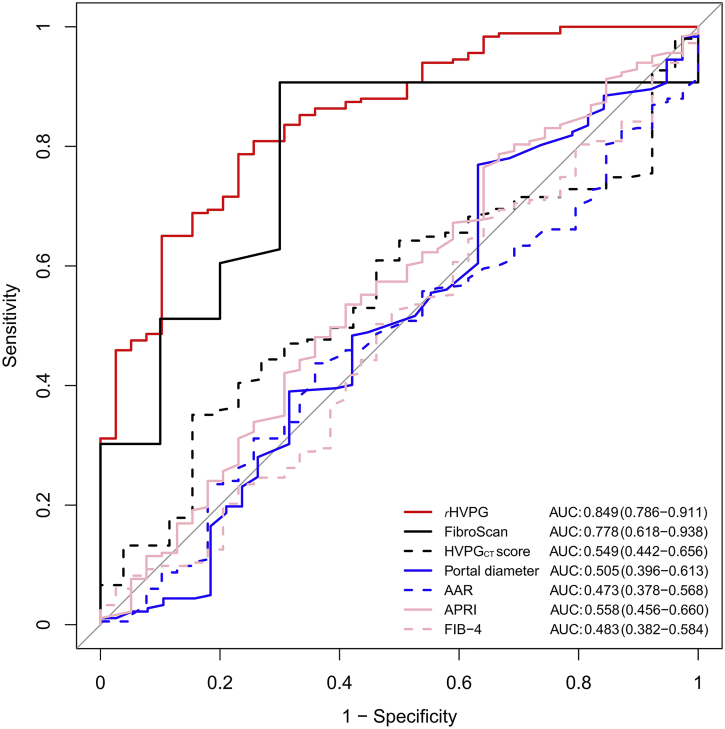
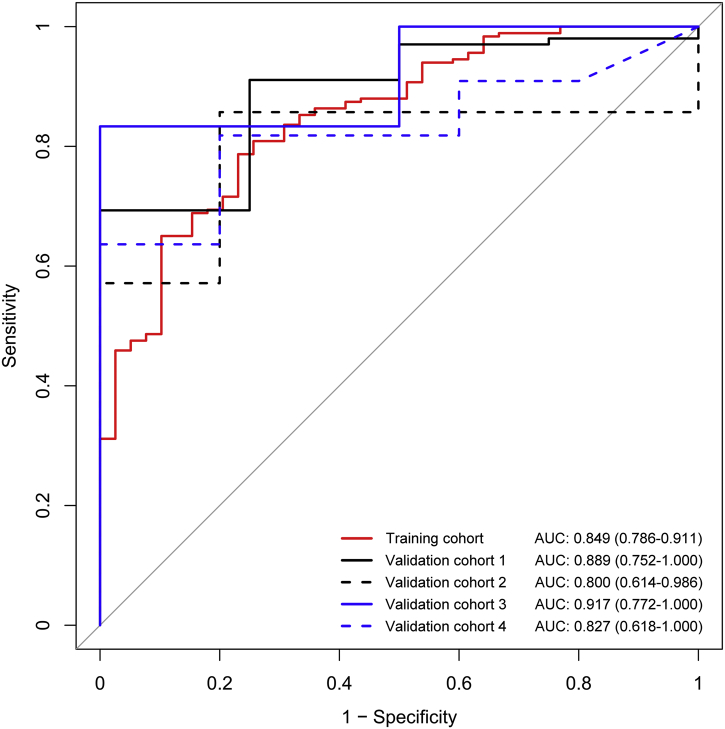
Clinically significant portal hypertension (CSPH) is associated with an incremental risk of esophageal varices and overt clinical decompensations. However, hepatic venous pressure gradient (HVPG) measurement, the gold standard for defining CSPH (HVPG≥10 mm Hg) is invasive and therefore not suitable for routine clinical practice. This study aims to develop and validate a radiomics-based model as a noninvasive method for accurate detection of CSPH in cirrhosis. The prospective multicenter diagnostic trial (CHESS1701, ClinicalTrials.gov identifier: NCT03138915) involved 385 patients with cirrhosis from five liver centers in China between August 2016 and September 2017. Patients who had both HVPG measurement and contrast-enhanced CT within 14 days prior to the catheterization were collected. The noninvasive radiomics model, termed rHVPG for CSPH was developed based on CT images in a training cohort consisted of 222 consecutive patients and the diagnostic performance was prospectively assessed in 163 consecutive patients in four external validation cohorts. rHVPG showed a good performance in detection of CSPH with a C-index of 0·849 (95%CI: 0·786-0·911). Application of rHVPG in four external prospective validation cohorts still gave excellent performance with the C-index of 0·889 (95%CI: 0·752-1·000, 0·800 (95%CI: 0·614-0·986), 0·917 (95%CI: 0·772-1·000), and 0·827 (95%CI: 0·618-1·000), respectively. Intraclass correlation coefficients for inter- and intra-observer agreement were 0·92-0·99 and 0·97-0·99, respectively. A radiomics signature was developed and prospectively validated as an accurate method for noninvasive detection of CSPH in cirrhosis. The tool of rHVPG assessment can facilitate the identification of CSPH rapidly when invasive transjugular procedure is not available.
Keywords: Hepatic venous pressure gradient; Liver cirrhosis; Noninvasive; Portal hypertension; Radiomics.
Copyright © 2018 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Virtual Hepatic Venous Pressure Gradient with CT Angiography (CHESS 1601): A Prospective Multicenter Study for the Noninvasive Diagnosis of Portal Hypertension.Radiology. 2019 Feb;290(2):370-377. doi: 10.1148/radiol.2018180425. Epub 2018 Nov 20. Radiology. 2019. PMID: 30457484
-
Deep Convolutional Neural Network-Aided Detection of Portal Hypertension in Patients With Cirrhosis.Clin Gastroenterol Hepatol. 2020 Dec;18(13):2998-3007.e5. doi: 10.1016/j.cgh.2020.03.034. Epub 2020 Mar 21. Clin Gastroenterol Hepatol. 2020. PMID: 32205218
-
Diagnosis of Clinically Significant Portal Hypertension Using CT- and MRI-based Vascular Model.Radiology. 2023 Apr;307(2):e221648. doi: 10.1148/radiol.221648. Epub 2023 Jan 31. Radiology. 2023. PMID: 36719293 Clinical Trial.
-
von Willebrand factor as a biomarker of clinically significant portal hypertension and severe portal hypertension: a systematic review and meta-analysis.BMJ Open. 2019 Aug 30;9(8):e025656. doi: 10.1136/bmjopen-2018-025656. BMJ Open. 2019. PMID: 31473610 Free PMC article.
-
Shear Wave Elastography as a Quantitative Biomarker of Clinically Significant Portal Hypertension: A Systematic Review and Meta-Analysis.AJR Am J Roentgenol. 2018 May;210(5):W185-W195. doi: 10.2214/AJR.17.18367. Epub 2018 Mar 23. AJR Am J Roentgenol. 2018. PMID: 29570374
Cited by
-
Clinical-radiomics nomogram for predicting esophagogastric variceal bleeding risk noninvasively in patients with cirrhosis.World J Gastroenterol. 2023 Feb 14;29(6):1076-1089. doi: 10.3748/wjg.v29.i6.1076. World J Gastroenterol. 2023. PMID: 36844133 Free PMC article.
-
Functional magnetic resonance imaging-based assessment of terlipressin vs. octreotide on renal function in cirrhotic patients with acute variceal bleeding (CHESS1903): study protocol of a multicenter randomized controlled trial.Ann Transl Med. 2019 Oct;7(20):586. doi: 10.21037/atm.2019.09.141. Ann Transl Med. 2019. PMID: 31807567 Free PMC article.
-
Artificial intelligence in the diagnosis of cirrhosis and portal hypertension.J Med Ultrason (2001). 2022 Jul;49(3):371-379. doi: 10.1007/s10396-021-01153-8. Epub 2021 Nov 17. J Med Ultrason (2001). 2022. PMID: 34787742 Review.
-
Evolution, progress, and prospects of research on transjugular intrahepatic portosystemic shunt applications.J Interv Med. 2021 Feb 20;4(2):57-61. doi: 10.1016/j.jimed.2021.02.001. eCollection 2021 May. J Interv Med. 2021. PMID: 34805949 Free PMC article. Review.
-
Role of artificial intelligence in hepatobiliary and pancreatic surgery.World J Gastrointest Surg. 2021 Jan 27;13(1):7-18. doi: 10.4240/wjgs.v13.i1.7. World J Gastrointest Surg. 2021. PMID: 33552391 Free PMC article. Review.
References
-
- Tsochatzis E.A., Bosch J., Burroughs A.K. Liver cirrhosis. Lancet. 2014;383(9930):1749–1761. - PubMed
-
- Garcia-Tsao G., Bosch J. Management of varices and variceal hemorrhage in cirrhosis. N Engl J Med. 2010;362(9):823–832. - PubMed
-
- García-Pagán J.C., Caca K., Bureau C. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med. 2010;362(25):2370–2379. - PubMed
-
- Bosch J., Abraldes J.G., Berzigotti A. The clinical use of HVPG measurements in chronic liver disease. Nat Rev Gastroenterol Hepatol. 2009;6(10):573–582. - PubMed
-
- Garcia-Tsao G., Abraldes J.G., Berzigotti A. Portal hypertensive bleeding in cirrhosis: risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology. 2017;65:310–335. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
