

Canakinumab in patients with systemic juvenile idiopathic arthritis and active systemic features: results from the 5-year long-term extension of the phase III pivotal trials
- PMID: 30269054
- PMCID: PMC6241618
- DOI: 10.1136/annrheumdis-2018-213150
Canakinumab in patients with systemic juvenile idiopathic arthritis and active systemic features: results from the 5-year long-term extension of the phase III pivotal trials
Abstract
Objectives: To evaluate the long-term efficacy and safety of canakinumab in patients with active systemic juvenile idiopathic arthritis (JIA).
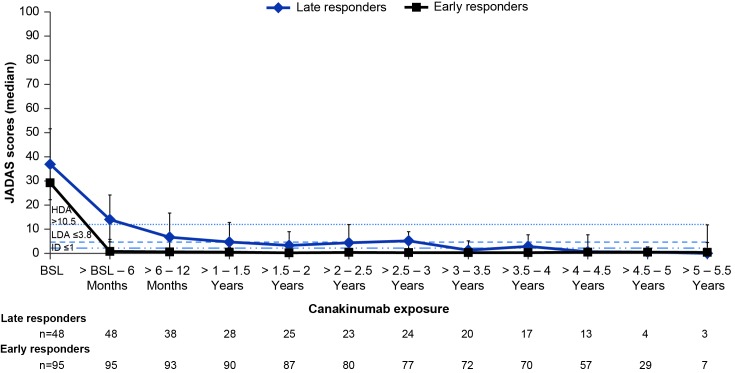
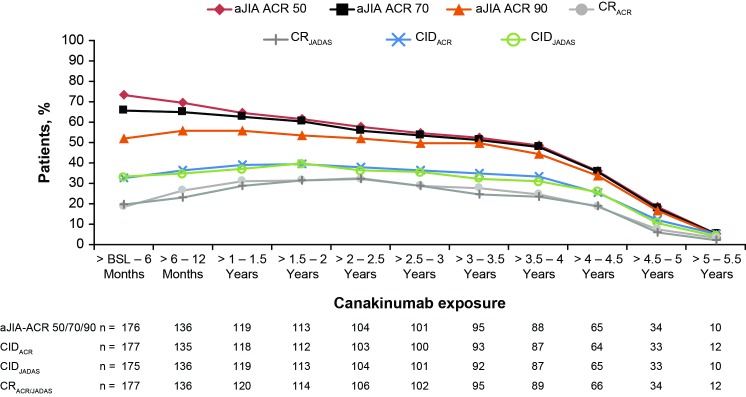
Methods: Patients (2-19 years) entered two phase III studies and continued in the long-term extension (LTE) study. Efficacy assessments were performed every 3 months, including adapted JIA American College of Rheumatology (aJIA-ACR) criteria, Juvenile Arthritis Disease Activity Score (JADAS) and ACR clinical remission on medication criteria (CRACR). Efficacy analyses are reported as per the intent-to-treat population.
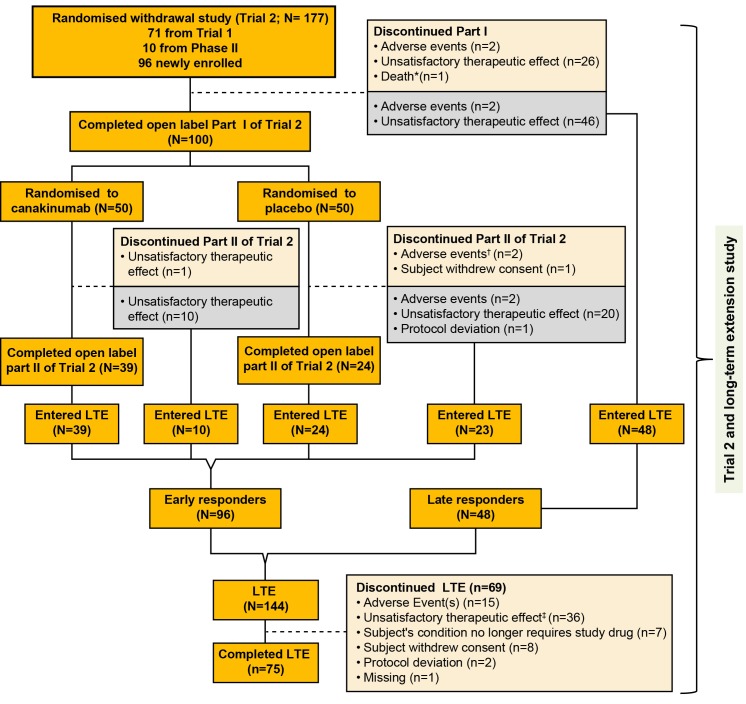
Results: 144 of the 177 patients (81%) enrolled in the core study entered the LTE. Overall, 75 patients (42%) completed and 102 (58%) discontinued mainly for inefficacy (63/102, 62%), with higher discontinuation rates noted in the late responders group (n=25/31, 81%) versus early responders (n=11/38, 29%). At 2 years, aJIA-ACR 50/70/90 response rates were 62%, 61% and 54%, respectively. CRACR was achieved by 20% of patients at month 6; 32% at 2 years. A JADAS low disease activity score was achieved by 49% of patients at 2 years. Efficacy results were maintained up to 5 years. Of the 128/177 (72.3%) patients on glucocorticoids, 20 (15.6%) discontinued and 28 (22%) tapered to 0.150 mg/kg/day. Seven patients discontinued canakinumab due to CR. There were 13 macrophage activation syndrome (three previously reported) and no additional deaths (three previously reported). No new safety findings were observed.
Conclusion: Response to canakinumab treatment was sustained and associated with substantial glucocorticoid dose reduction or discontinuation and a relatively low retention-on-treatment rate. No new safety findings were observed on long-term use of canakinumab.
Trial registration numbers: NCT00886769, NCT00889863, NCT00426218 and NCT00891046.
Keywords: canakinumab; clinical trial; interleukin-1β; long-term extension; systemic juvenile idiopathic arthritis..
© Author(s) (or their employer(s)) 2018. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: NR: consultant and speaker’s bureaus from AbbVie, Ablynx, Amgen, AstraZeneca, Baxalta Biosimilars, Biogen Idec, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli-Lilly, EMD Serono, Gilead Sciences, Janssen, MedImmune, Novartis, Pfizer, R-Pharm, Roche, Sanofi, Servier, Takeda; NR works as a full-time public employee of the public hospital Istituto Giannina Gaslini, which has received contributions from Bristol-Myers Squibb, Hoffman-La Roche, Janssen, Novartis, Pfizer, Sobi for the coordination activity of the PRINTO network. HIB: consultant: AstraZeneca, Bristol-Myers Squibb, Genentech, Janssen, Novartis, Pfizer, Sanofi, Takeda; speaker’s bureaus: Genentech, Novartis Pierre Quartier; has received consultant fees from Novimmune, Novartis and SOBI; has received speaker’s bureaus from Abbvie, BMS, Chugai-Roche, Lilly, Novartis, Pfizer and Sobi; has acted as coordinator or investigator in clinical trials for Abbvie, BMS, Chugai-Roche, Novartis, Sanofi, Sobi; has acted as member of a data monitoring board committee for Sanofi. NMW has received grant/research support from AbbVie; has received consultant fees from AbbVie, Sobi and Novartis. GH has received speaker’s bureaus from AbbVie, Boehringer Ingelheim, Chugai, MSD, Novartis, Pfizer, Roche and Sobi; has received scientific grants from AbbVie, Chugai, MSD, Novartis, Pfizer and Roche. OK has received speaker’s bureaus from Novartis, Roche, Pfizer and Abbvie. RS has received consultant fees from Novartis, Sobi and Novimmune. JLA has received consultant fees and speaker’s bureaus from AbbVie, Gebro, Novartis, Pfizer, Roche, Sanofi and Sobi. RC has received consultant fees and speaker’s bureaus from Bristol-Myers Squibb, Janssen, Novartis, Pfizer, Sanofi, Roche, Lilly and GlaxoSmithKline. HEF has acted as member of advisory boards for AbbVie, Novartis, Pfizer, Sanofi and Sobi; has received unrestricted educational bursaries from Pfizer, Genzyme, BioMarin and Sobi to develop educational resources for healthcare professionals. DF has received grant/research support from Pfizer and Novartis; has received consultant fees from Novartis, Pfizer, Chugai-Roche and Sobi; has received speaker’s bureaus from Novartis. SCR has received grants for clinical research from Novartis. AVR has received honoraria and participated in Advisory Boards for Novartis. RT has received lecture fees from Pfizer and Bristol-Myers Squibb. JL received fees from Novartis for conducting the statistical analysis. EV is an employee of Novartis Pharma, Basel, Switzerland. AM has no conflicts of interest to declare since March 2016 when he became the Scientific Director of the Istituto Giannina Gaslini, because this role does not allow him to render private consultancy resulting in personal income; consultant on behalf of the Istituto Giannina Gaslini: AbbVie, Boehringer, Novartis, R-Pharm. Istituto Giannina Gaslini has received contributions from Bristol-Myers Squibb, Hoffman-La Roche, Janssen, Novartis, Pfizer, Sobi for the coordination activity of the PRINTO network. DJL has received grant/research support from AbbVie, Bristol-Myers Squibb, NIH, Pfizer, Roche; speaker’s bureaus from Genentech; consultant of AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Genentech, GlaxoSmithKline, Janssen, Johnson & Johnson, Novartis, Takeda, UCB. EU, FC, JB, MF, MF-d, RB and TC have nothing to disclose.
Figures
References
-
- Quartier P, Allantaz F, Cimaz R, et al. . A multicentre, randomised, double-blind, placebo-controlled trial with the interleukin-1 receptor antagonist anakinra in patients with systemic-onset juvenile idiopathic arthritis (ANAJIS trial). Ann Rheum Dis 2011;70:747–54. 10.1136/ard.2010.134254 - DOI - PMC - PubMed
