

United Kingdom Diabetic Retinopathy Electronic Medical Record (UK DR EMR) Users Group: report 4, real-world data on the impact of deprivation on the presentation of diabetic eye disease at hospital services
- PMID: 30269098
- PMCID: PMC6582816
- DOI: 10.1136/bjophthalmol-2018-312568
United Kingdom Diabetic Retinopathy Electronic Medical Record (UK DR EMR) Users Group: report 4, real-world data on the impact of deprivation on the presentation of diabetic eye disease at hospital services
Abstract
Aim: To assess the impact of deprivation on diabetic retinopathy presentation and related treatment interventions, as observed within the UK hospital eye service.
Methods: This is a multicentre, national diabetic retinopathy database study with anonymised data extraction across 22 centres from an electronic medical record system. The following were the inclusion criteria: all patients with diabetes and a recorded, structured diabetic retinopathy grade. The minimum data set included, for baseline, age and Index of Multiple Deprivation, based on residential postcode; and for all time points, visual acuity, ETDRS grading of retinopathy and maculopathy, and interventions (laser, intravitreal therapies and surgery). The main outcome measures were (1) visual acuity and binocular visual state, and (2) presence of sight-threatening complications and need for early treatment.
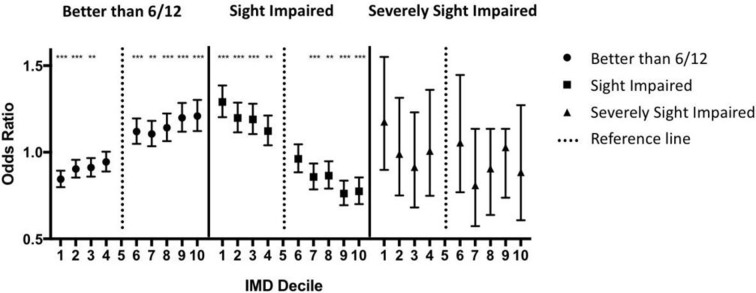
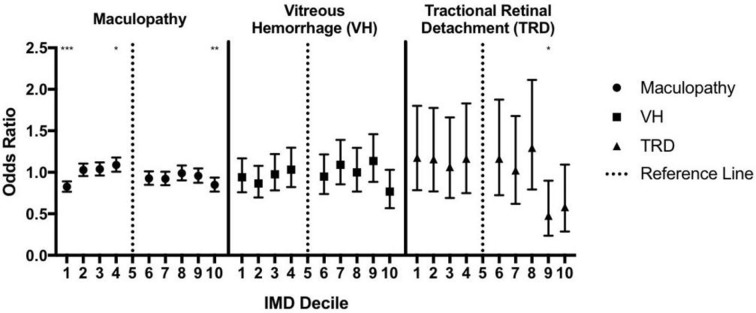
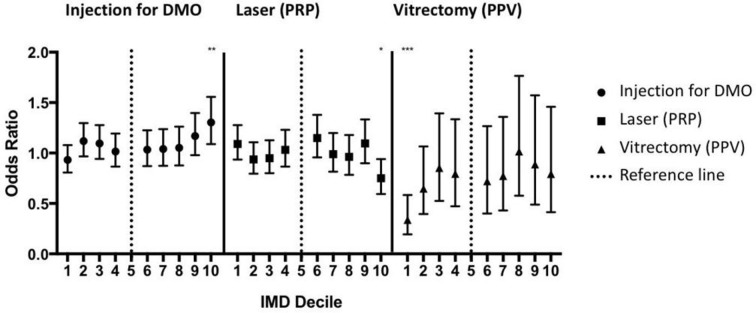
Results: 79 775 patients met the inclusion criteria. Deprivation was associated with later presentation in patients with diabetic eye disease: the OR of being sight-impaired at entry into the hospital eye service (defined as 6/18 to better than 3/60 in the better seeing eye) was 1.29 (95% CI 1.20 to 1.39) for the most deprived decile vs 0.77 (95% CI 0.70 to 0.86) for the least deprived decile; the OR for being severely sight-impaired (3/60 or worse in the better seeing eye) was 1.17 (95% CI 0.90 to 1.55) for the most deprived decile vs 0.88 (95% CI 0.61 to 1.27) for the least deprived decile (reference=fifth decile in all cases). There is also variation in sight-threatening complications at presentation and treatment undertaken: the least deprived deciles had lower chance of having a tractional retinal detachment (OR=0.48 and 0.58 for deciles 9 and 10, 95% CI 0.24 to 0.90 and 0.29 to 1.09, respectively); in terms of accessing treatment, the rate of having a vitrectomy was lowest in the most deprived cohort (OR=0.34, 95% CI 0.19 to 0.58).
Conclusions: This large real-world study suggests that first presentation at a hospital eye clinic with visual loss or sight-threatening diabetic eye disease is associated with deprivation. These initial hospital visits represent the first opportunities to receive treatment and to formally engage with support services. Such patients are more likely to be sight-impaired or severely sight-impaired at presentation, and may need additional resources to engage with the hospital eye services over complex treatment schedules.
Keywords: diabetes; electronic medical record.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: CAE has received consultancy fees from Medisoft. LD has undertaken advisory board work previously for Novartis, Bayer, Allergan, Alimera, Alcon, Oraya and Thrombogenics; and received speaker fees from Bayer, Novartis and Alimera, and travel grants from Novartis, Bayer and Allergan. HE has undertaken advisory board work for Novartis and Bayer; received speaker fees from Novartis, and travel grants from Novartis, Bayer and Allergan. RM has undertaken advisory board work for Alimera; received speaker fees from Bayer and Alcon; and obtained travel and educational grants from Novartis and Bayer. UC has undertaken advisory board work for Allergan, Bayer, Novartis and Roche; and received speaker fees from Heidelberg and Zeiss. SP has undertaken advisory board work and received travel grants from Bayer, Alimera, Allergan and Novartis. DPC has received speaker fees from Allergan and Santen. DAS has received consultancy fees from Big Picture Medical; speaker fees from Bayer, Novartis, Allergan and Haag-Streit; and travel grants from Bayer and Allergan. AnL has received travel grants from Bayer and Allergan. CB has undertaken advisory board work for Alimera, Bayer and Novartis, and received travel support/speaker fees from Alimera, Bayer and Novartis. FG has undertaken advisory board work for Novartis, Bayer, Allergan, Alimera, Alcon and Roche; received speaker fees from Bayer, Novartis, Alimera and Allergan, and travel grants from Bayer and Allergan. RK has undertaken advisory board work for Alimera; received speaker fees from Novartis, and travel grants from Novartis, Bayer, Alimera and Allergan. TA has undertaken advisory board work for Bayer; received speaker fees from Novartis, and travel grants from Novartis and Bayer. HP has received travel grants from Bayer and Alimera. RA has received travel grants from Novartis, Bayer and Allergan. VK has undertaken advisory board work for Polyphotonix and received speaker fees from Heidelberg. ND has undertaken advisory board work for Novartis and Allergan; received speaker fees for Novartis and Bayer; and received travel grants from Novartis, Allergan and Bayer.
Figures
References
-
- World Health Organization. Closing the gap in a generation: health equity through action on the social determinants of health: commission on social determinants of health final report. Geneva: World Health Organization, 2008.
-
- Townsend P. Deprivation. J Soc Policy 1987;16:125 10.1017/S0047279400020341 - DOI
-
- Buck D, Maguire D. Inequalities in Life Expectancy: Changes Over Time and Implications for Policy. 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous