

Effect and Safety of Meropenem-Vaborbactam versus Best-Available Therapy in Patients with Carbapenem-Resistant Enterobacteriaceae Infections: The TANGO II Randomized Clinical Trial
- PMID: 30270406
- PMCID: PMC6249182
- DOI: 10.1007/s40121-018-0214-1
Effect and Safety of Meropenem-Vaborbactam versus Best-Available Therapy in Patients with Carbapenem-Resistant Enterobacteriaceae Infections: The TANGO II Randomized Clinical Trial
Abstract
Introduction: Treatment options for carbapenem-resistant Enterobacteriaceae (CRE) infections are limited and CRE infections remain associated with high clinical failure and mortality rates, particularly in vulnerable patient populations. A Phase 3, multinational, open-label, randomized controlled trial (TANGO II) was conducted from 2014 to 2017 to evaluate the efficacy/safety of meropenem-vaborbactam monotherapy versus best available therapy (BAT) for CRE.
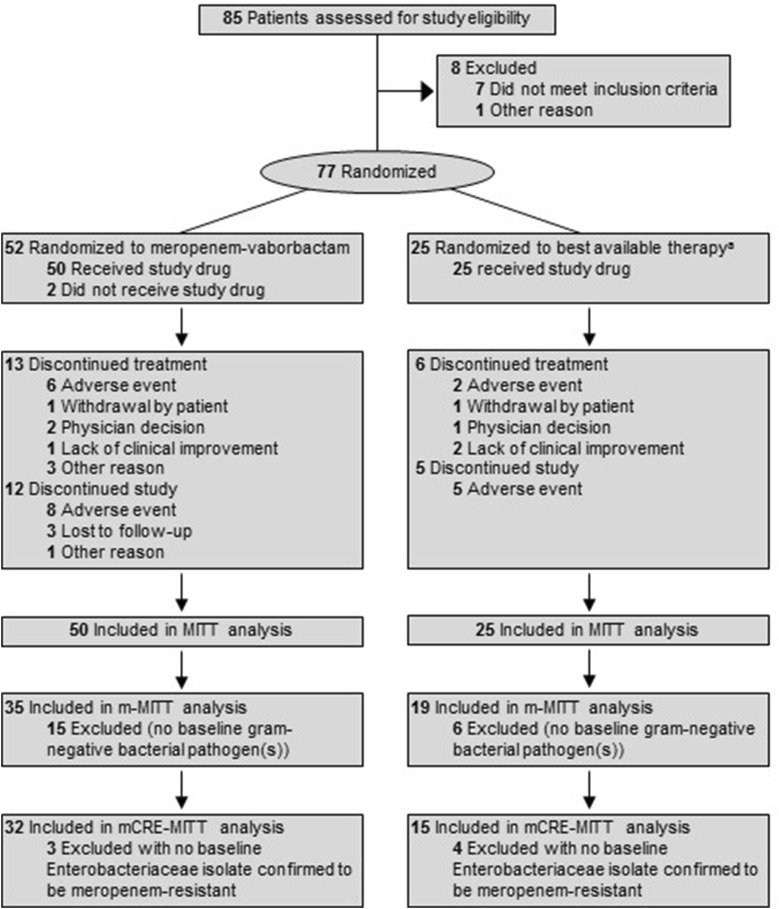
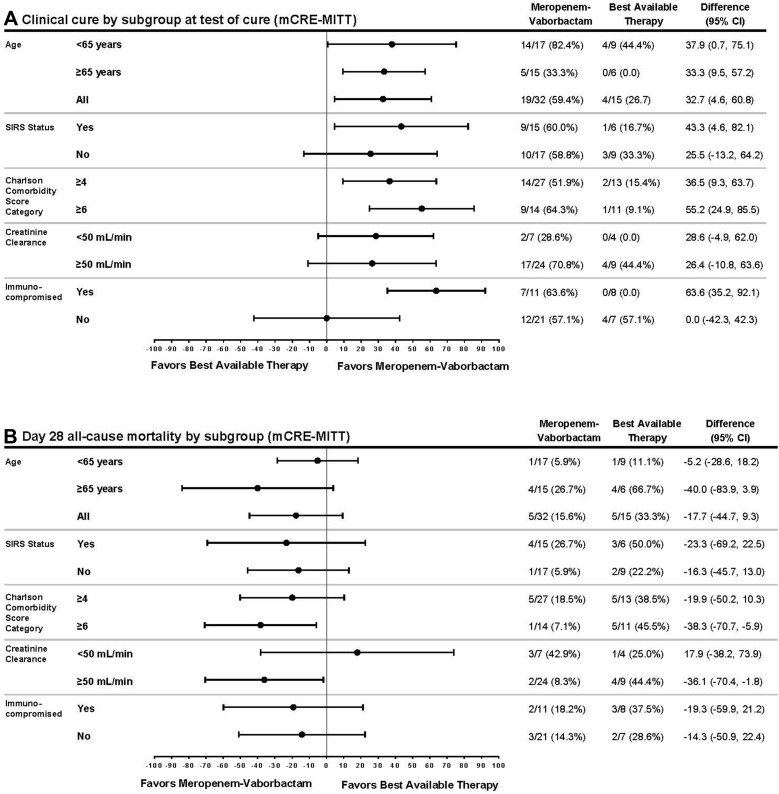
Methods: A total of 77 patients with confirmed/suspected CRE infection (bacteremia, hospital-acquired/ventilator-associated bacterial pneumonia, complicated intra-abdominal infection, complicated urinary tract infection/acute pyelonephritis) were randomized, and 47 with confirmed CRE infection formed the primary analysis population (microbiologic-CRE-modified intent-to-treat, mCRE-MITT). Eligible patients were randomized 2:1 to meropenem-vaborbactam (2 g/2 g over 3 h, q8h for 7-14 days) or BAT (mono/combination therapy with polymyxins, carbapenems, aminoglycosides, tigecycline; or ceftazidime-avibactam alone). Efficacy endpoints included clinical cure, Day-28 all-cause mortality, microbiologic cure, and overall success (clinical cure + microbiologic eradication). Safety endpoints included adverse events (AEs) and laboratory findings.
Results: Within the mCRE-MITT population, cure rates were 65.6% (21/32) and 33.3% (5/15) [95% confidence interval (CI) of difference, 3.3% to 61.3%; P = 0.03)] at End of Treatment and 59.4% (19/32) and 26.7% (4/15) (95% CI of difference, 4.6% to 60.8%; P = 0.02) at Test of Cure;.Day-28 all-cause mortality was 15.6% (5/32) and 33.3% (5/15) (95% CI of difference, - 44.7% to 9.3%) for meropenem-vaborbactam versus BAT, respectively. Treatment-related AEs and renal-related AEs were 24.0% (12/50) and 4.0% (2/50) for meropenem-vaborbactam versus 44.0% (11/25) and 24.0% (6/25) for BAT. Exploratory risk-benefit analyses of composite clinical failure or nephrotoxicity favored meropenem-vaborbactam versus BAT (31.3% [10/32] versus 80.0% [12/15]; 95% CI of difference, - 74.6% to - 22.9%; P < 0.001).
Conclusions: Monotherapy with meropenem-vaborbactam for CRE infection was associated with increased clinical cure, decreased mortality, and reduced nephrotoxicity compared with BAT.
Clinical trials registration: NCT02168946.
Funding: The Medicines Company.
Keywords: Best available therapy; Carbapenem-resistant Enterobacteriaceae; Meropenem–vaborbactam; Randomized clinical trial; TANGO II.
Figures
References
-
- Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. https://www.cdc.gov/drugresistance/threat-report-2013/index.html. Accessed 27 Aug 2017.
-
- World Health Organization. Global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. http://www.who.int/medicines/publications/global-priority-list-antibioti.... Accessed 5 Sep 2017.
-
- European Commission. A European One Health action plan against antimicrobial resistance (AMR). https://ec.europa.eu/health/amr/action_eu_en. Accessed 5 Sep 2017.
-
- The Pew Charitable Trusts. GAIN: how a new law is stimulating the development of antibiotics. http://www.pewtrusts.org/en/research-and-analysis/issue-briefs/2013/11/0.... Accessed 5 Sep 2017.
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
