Outcome of Ventriculosubgaleal Shunt in the Management of Infectious and Non-infectious Hydrocephalus in Pre-term Infants
- PMID: 30271465
- PMCID: PMC6144600
- DOI: 10.4103/JPN.JPN_41_18
Outcome of Ventriculosubgaleal Shunt in the Management of Infectious and Non-infectious Hydrocephalus in Pre-term Infants
Abstract
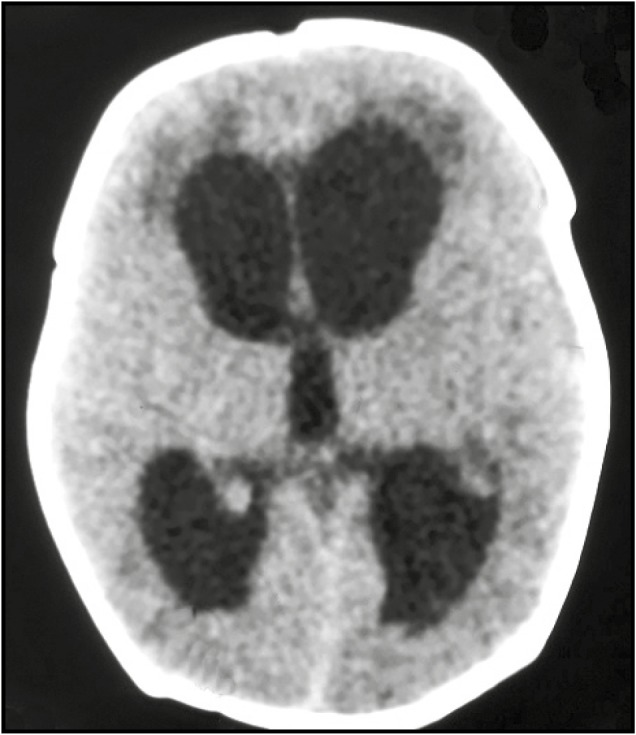
Background: Hydrocephalus in premature infants is an onerous disease. In such situations, choosing the best option for cerebrospinal fluid (CSF) diversion is difficult. Ventriculosubgaleal shunt is an effective method of temporary CSF diversion in such situations. In this retrospective study, we compare the outcome of ventriculosubgaleal shunt in premature infants with hydrocephalus of infectious and noninfectious etiology.
Materials and methods: All premature children with hydrocephalus secondary to various etiologies who underwent ventriculosubgaleal shunt were studied. The participants were grouped into two depending upon the etiology of hydrocephalus: Group 1 (infectious) and Group 2 (non-infectious). The primary outcome was a successful conversion to ventriculoperitoneal shunt (VPS) and the secondary outcome was mortality. Data were entered into statistical software SPSS version 16 and appropriate statistical analysis was performed to conclude any statistical significance between groups.
Results: The study included 16 infants among whom 9 were in the infectious group and 7 in the non-infectious group. Primary end point of conversion to VPS was achieved in 55.5% of patients in group 1 and 85.7% in group 2. The secondary end point, i.e., mortality was observed in 44.4% of patients in group 1 and 14.2% in group 2. The average duration during which this was achieved was 40 days (range 20-60 days) in group 1 and 25 days (range 20-30 days) in group 2.
Conclusion: Ventriculosubgaleal shunt is a safe and effective procedure in infants awaiting definitive VPS for hydrocephalus of infectious as well as noninfectious origin. There was no statistical difference in the rate of successful conversion to a permanent VPS from ventriculosubgaleal shunt in hydrocephalus of either etiologies. Complications and time for successful conversion were more in postmeningitic hydrocephalus.
Keywords: Hydrocephalus; premature infants; ventriculosubgaleal shunt.
Conflict of interest statement
There are no conflicts of interest.
Figures


Similar articles
-
Ventriculosubgaleal shunt as a proposed technique for post-infectious hydrocephalus.Childs Nerv Syst. 2022 Nov;38(11):2155-2162. doi: 10.1007/s00381-022-05661-x. Epub 2022 Oct 10. Childs Nerv Syst. 2022. PMID: 36214898 Free PMC article.
-
Ventriculosubgaleal shunts for posthemorrhagic hydrocephalus in premature infants.Pediatr Neurosurg. 2005 Jul-Aug;41(4):178-85. doi: 10.1159/000086558. Pediatr Neurosurg. 2005. PMID: 16088252
-
Comparison between Ventriculosubgaleal Shunt and Extraventricular Drainage to Treat Acute Hydrocephalus in Adults.Asian J Neurosurg. 2017 Oct-Dec;12(4):659-663. doi: 10.4103/ajns.AJNS_122_16. Asian J Neurosurg. 2017. PMID: 29114279 Free PMC article.
-
Ventriculosubgaleal shunting-a comprehensive review and over two-decade surgical experience.Childs Nerv Syst. 2018 Sep;34(9):1639-1642. doi: 10.1007/s00381-018-3887-6. Epub 2018 Jul 12. Childs Nerv Syst. 2018. PMID: 30003327 Review.
-
Ventriculosubgaleal shunting--a strategy to reduce the incidence of shunt revisions and slit ventricles: an institutional experience and review of the literature.Pediatr Neurosurg. 2011;47(2):99-107. doi: 10.1159/000330539. Epub 2011 Sep 13. Pediatr Neurosurg. 2011. PMID: 21921577 Review.
Cited by
-
Ventriculosubgaleal shunt as a proposed technique for post-infectious hydrocephalus.Childs Nerv Syst. 2022 Nov;38(11):2155-2162. doi: 10.1007/s00381-022-05661-x. Epub 2022 Oct 10. Childs Nerv Syst. 2022. PMID: 36214898 Free PMC article.
-
Comparative study between ventriculosubgaleal shunt and external ventricular drain for management of post infective hydrocephalus among pediatrics.Childs Nerv Syst. 2024 Jun;40(6):1771-1776. doi: 10.1007/s00381-024-06344-5. Epub 2024 Mar 5. Childs Nerv Syst. 2024. PMID: 38441628 Free PMC article. Clinical Trial.
-
Surgical management of intraventricular hemorrhage and posthemorrhagic hydrocephalus in premature infants - single center experience.Front Pediatr. 2025 Aug 7;13:1610697. doi: 10.3389/fped.2025.1610697. eCollection 2025. Front Pediatr. 2025. PMID: 40852412 Free PMC article.
-
Outcome of Ventriculosubgaleal Shunt in Management of Hydrocephalus.J Pediatr Neurosci. 2019 Apr-Jun;14(2):105. doi: 10.4103/jpn.JPN_139_18. J Pediatr Neurosci. 2019. PMID: 31516632 Free PMC article. No abstract available.
-
Germinal Matrix-Intraventricular Hemorrhage: A Tale of Preterm Infants.Int J Pediatr. 2021 Mar 16;2021:6622598. doi: 10.1155/2021/6622598. eCollection 2021. Int J Pediatr. 2021. PMID: 33815512 Free PMC article. Review.
References
-
- Rahman S, Teo C, Morris W, Lao D, Boop FA. Ventriculosubgaleal shunt: a treatment option for progressive posthemorrhagic hydrocephalus. Childs Nerv Syst. 1995;11:650–4. - PubMed
-
- Tubbs RS, Smyth MD, Wellons JC, 3rd, Blount JP, Grabb PA, Oakes WJ. Alternative uses for the subgaleal shunt in pediatric neurosurgery. Pediatr Neurosurg. 2003;39:22–4. - PubMed
-
- Cornips E, Van Calenbergh F, Plets C, Devlieger H, Casaer P. Use of external drainage for posthemorrhagic hydrocephalus in very low birth weight premature infants. Childs Nerv Syst. 1997;13:369–74. - PubMed
-
- Lam HP, Heilman CB. Ventricular access device versus ventriculosubgaleal shunt in post hemorrhagic hydrocephalus associated with prematurity. J Matern Fetal Neonatal Med. 2009;22:1097–101. - PubMed
-
- Wang JY, Amin AG, Jallo GI, Ahn ES. Ventricular reservoir versus ventriculosubgaleal shunt for posthemorrhagic hydrocephalus in preterm infants: infection risks and ventriculoperitoneal shunt rate. J Neurosurg Pediatr. 2014;14:447–54. - PubMed