

Practice Guideline
doi: 10.1210/jc.2018-01865.
Congenital Adrenal Hyperplasia Due to Steroid 21-Hydroxylase Deficiency: An Endocrine Society Clinical Practice Guideline
Affiliations
- PMID: 30272171
- PMCID: PMC6456929
- DOI: 10.1210/jc.2018-01865
Item in Clipboard
Practice Guideline
Congenital Adrenal Hyperplasia Due to Steroid 21-Hydroxylase Deficiency: An Endocrine Society Clinical Practice Guideline
J Clin Endocrinol Metab.
.
Erratum in
-
CORRIGENDUM FOR "Congenital Adrenal Hyperplasia Due to Steroid 21-Hydroxylase Deficiency: An Endocrine Society* Clinical Practice Guideline".J Clin Endocrinol Metab. 2019 Jan 1;104(1):39-40. doi: 10.1210/jc.2018-02371. J Clin Endocrinol Metab. 2019. PMID: 30407499 Free PMC article. No abstract available.
Abstract
Objective: To update the congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency clinical practice guideline published by the Endocrine Society in 2010.
Conclusions: The writing committee presents updated best practice guidelines for the clinical management of congenital adrenal hyperplasia based on published evidence and expert opinion with added considerations for patient safety, quality of life, cost, and utilization.
Figures
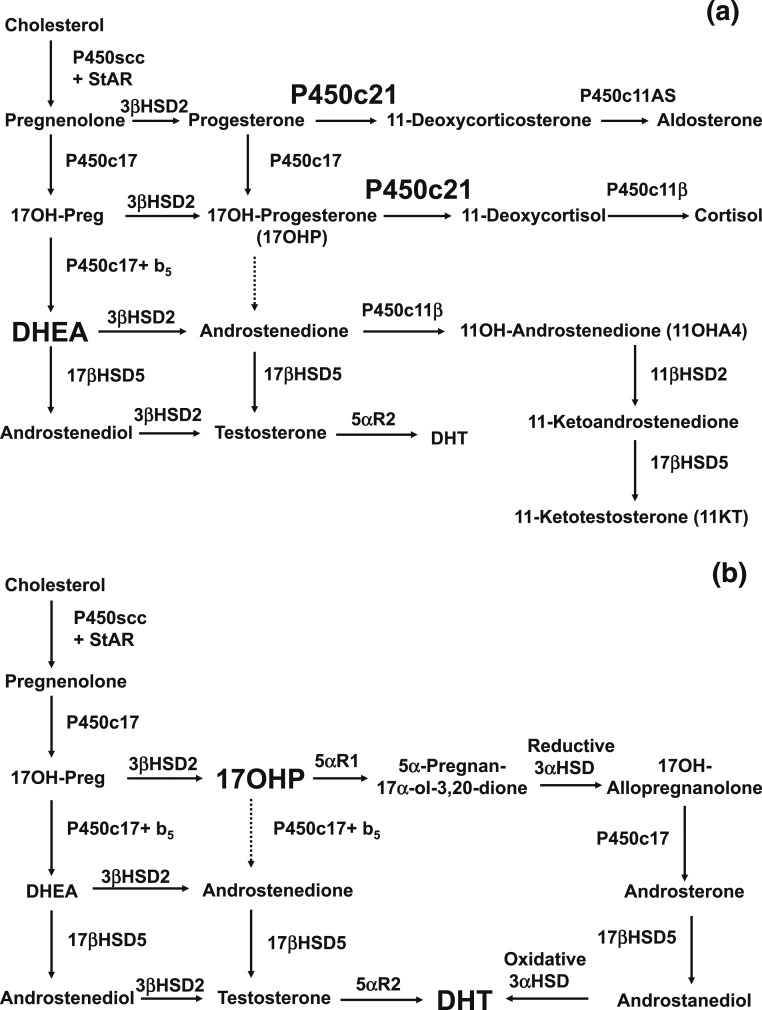
(a) Normal fetal adrenal steroidogenesis. Because the fetal adrenal has low levels of 3β-hydroxysteroid dehydrogenase, most steroidogenesis is directed toward dehydroepiandrosterone (DHEA) and thence to DHEA sulfate, but small amounts of steroids enter the pathways toward aldosterone and cortisol. The adrenal 21-hydroxylase P450c21 is essential in both pathways. The adrenal can synthesize small amounts of testosterone via 17βHSD5 (AKR1C3). Included to the lower right is the 11-oxyandrogen pathway, in which androstenedione is converted in the adrenal to 11β-hydroxyandrostenedione (11OHA4) and then in the adrenal and/or peripheral tissues to 11-ketoandrostenedione and ultimately 11-ketotestosterone (11KT). The production of 11OHA4 and 11KT is an important pathway in postnatal life and may also occur in the fetal adrenal. (b) In the absence of the 21-hydroxylase activity of P450c21, three pathways lead to androgens. First, the pathway from cholesterol to DHEA remains intact. Although much DHEA is inactivated to DHEA sulfate, the increased production of DHEA will lead to some DHEA being converted to testosterone and dihydrotestosterone (DHT). Second, although minimal amounts of 17OHP are converted to androstenedione in the normal adrenal, the massive amounts of 17OHP produced in CAH permit some 17OHP to be converted to androstenedione and then to testosterone. Third, the alternative pathway depends on the 5α and 3α reduction of 17OHP to 17OH-allopregnanolone. This steroid is readily converted to androstanediol, which can then be oxidized to DHT by an oxidative 3α-hydroxysteroid dehydrogenase (3αHSD) enzyme. The role of the alternative pathway in CAH is evidenced by increased levels of metabolites of its unique steroidal intermediates in the urine of infants, children, and adults with CAH (26).
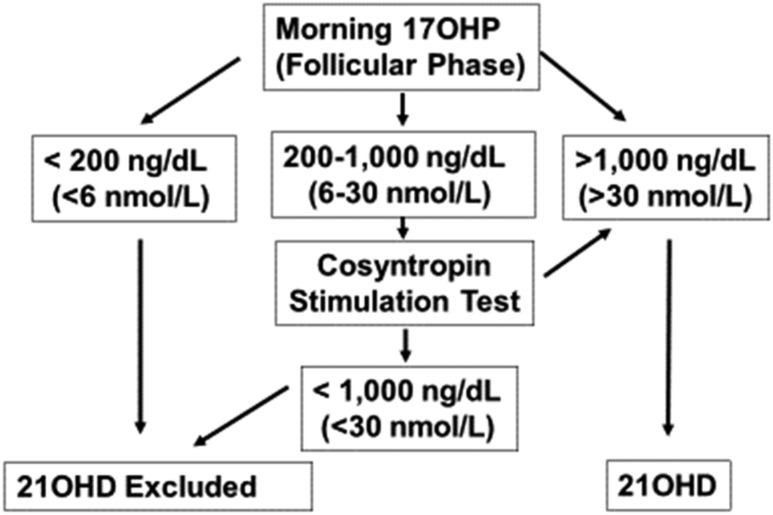
Diagnosis of 21OHD. Reference standards for hormonal diagnosis were derived from Refs. (170, 171, 173, 174). These diagnostic thresholds appear similar for LC-MS/MS assays from limited data (175). Note that randomly measured 17OHP levels can be normal in NCCAH; hence, 17OHP levels should be screened in the early morning (before 8 am ). For menstruating females, steroid measurements should be obtained in the follicular phase and may differ depending on the assay employed. Individuals with classic CAH, including both salt-wasting and simple virilizing forms of 21OHD, typically have unstimulated 17OHP values of several thousand. Note that it is sometimes difficult to distinguish clinically between non–salt-wasting classic and nonclassic forms of CAH.
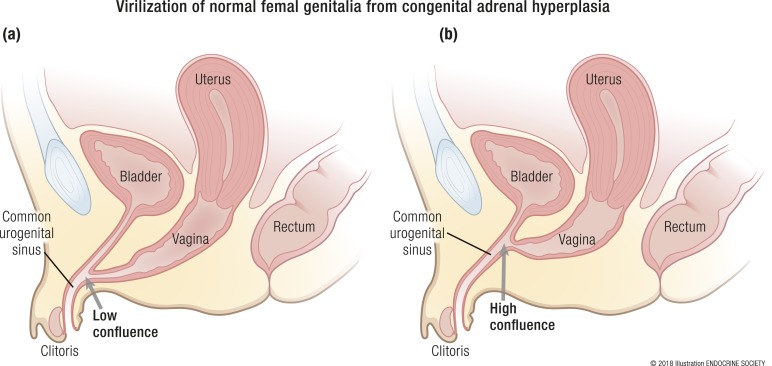
Lower urogenital anatomy of mild and severe CAH. (a and b) The lower urogenital anatomy of mild and severe CAH is shown. Note the low confluence in (a), where the vagina and urethra meet close to the skin, in contrast to (b), where the confluence of the vagina and urethra is close to the bladder neck. [Illustration ENDOCRINE SOCIETY]
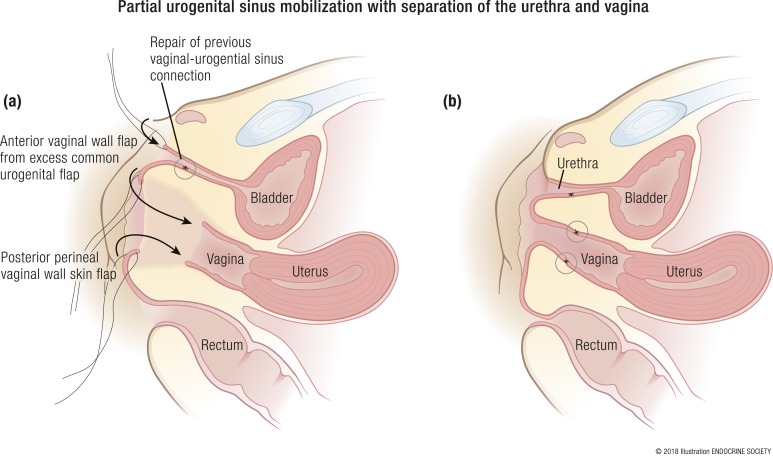
Partial urogenital mobilization with separation of the urethra and vagina. (a and b) Schematic of partial urogenital sinus mobilization where normal female anatomy is restored. Note the separation in (a) of the vagina and urethra with preparation of the excess common urogenital sinus to form the anterior vaginal wall by anastomosis to the normal anterior vaginal wall (b) and preparation of the posterior perineal skin flap (a) to form the posterior vaginal wall (b). [Illustration ENDOCRINE SOCIETY]
Comment in
-
Response to Letter to the Editor: "Congenital Adrenal Hyperplasia Due to Steroid 21-Hydroxylase Deficiency: An Endocrine Society Clinical Practice Guideline".J Clin Endocrinol Metab. 2019 Jun 1;104(6):1928. doi: 10.1210/jc.2018-02629. J Clin Endocrinol Metab. 2019. PMID: 30561699 Free PMC article. No abstract available.
-
Letter to the Editor: "Congenital Adrenal Hyperplasia Due to Steroid 21-Hydroxylase Deficiency: An Endocrine Society Clinical Practice Guideline".J Clin Endocrinol Metab. 2019 Jun 1;104(6):1926-1927. doi: 10.1210/jc.2018-02529. J Clin Endocrinol Metab. 2019. PMID: 30561707 No abstract available.
References
-
- Speiser PW, Azziz R, Baskin LS, Ghizzoni L, Hensle TW, Merke DP, Meyer-Bahlburg HFL, Miller WL, Montori VM, Oberfield SE, Ritzen M, White PC. Congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95(9):4133–4160. - PMC - PubMed
-
- Gruñieiro-Papendieck L, Chiesa A, Mendez V, Prieto L. Neonatal screening for congenital adrenal hyperplasia: experience and results in Argentina. J Pediatr Endocrinol Metab. 2008;21(1):73–78. - PubMed
-
- Shetty VB, Bower C, Jones TW, Lewis BD, Davis EA. Ethnic and gender differences in rates of congenital adrenal hyperplasia in Western Australia over a 21 year period. J Paediatr Child Health. 2012;48(11):1029–1032. - PubMed
-
- Gleeson HK, Wiley V, Wilcken B, Elliott E, Cowell C, Thonsett M, Byrne G, Ambler G. Two-year pilot study of newborn screening for congenital adrenal hyperplasia in New South Wales compared with nationwide case surveillance in Australia. J Paediatr Child Health. 2008;44(10):554–559. - PubMed
-
- Nascimento ML, Cristiano AN, Campos T, Ohira M, Cechinel E, Simoni G, Lee J, Linhares RM, Silva PC. Ten-year evaluation of a neonatal screening program for congenital adrenal hyperplasia. Arq Bras Endocrinol Metabol. 2014;58(7):765–771. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
