

Acetabular Retroversion and Decreased Posterior Coverage Are Associated With Sports-related Posterior Hip Dislocation in Adolescents
- PMID: 30272610
- PMCID: PMC6494309
- DOI: 10.1097/CORR.0000000000000514
Acetabular Retroversion and Decreased Posterior Coverage Are Associated With Sports-related Posterior Hip Dislocation in Adolescents
Abstract
Background: Leverage of the femoral head against the acetabular rim may lead to posterior hip dislocation during sports activities in hips with femoroacetabular impingement (FAI) deformity. Abnormal concavity of the femoral head and neck junction has been well described in association with posterior hip dislocation. However, acetabular morphology variations are not fully understood.
Questions/purposes: The purpose of this study was to compare the acetabular morphology in terms of acetabular version and coverage of the femoral head in adolescents who sustained a posterior hip dislocation during sports and recreational activities with a control group of patients without a history of hip disease matched by age and sex.
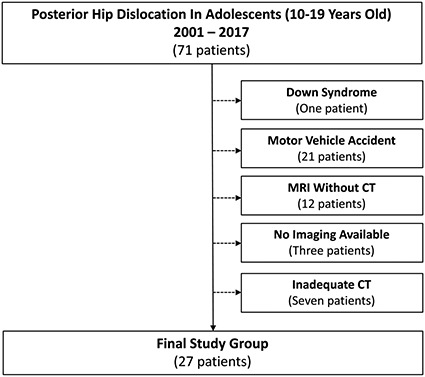
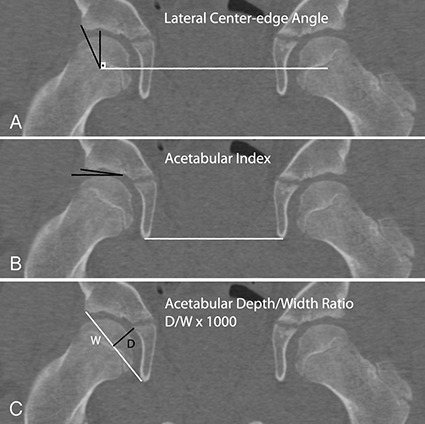
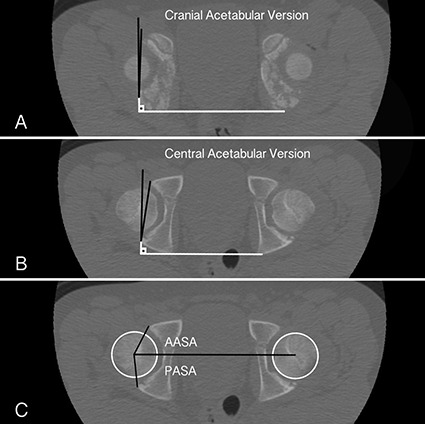
Methods: In this case-control study, we identified 27 adolescents with posterior hip dislocation sustained during sports or recreational activities who underwent a CT scan of the hips (study group) and matched them to patients without a history of hip disease being evaluated with CT for possible appendicitis (control group). Between 2001 and 2017, we treated 71 adolescents (aged 10-19 years old) for posterior hip dislocations. During the period in question, we obtained CT scans or MR images after closed reduction of a posterior hip dislocation. One patient was excluded because of a diagnosis of Down syndrome. Twenty-one patients who were in motor vehicle-related accidents were also excluded. Twelve patients were excluded because MRI was obtained instead of CT. Finally, three patients with no imaging after reduction and seven patients with inadequate CT reformatting were excluded. Twenty-seven patients (38%) had CT scans of suitable quality for analysis, and these 27 patients constituted the study group. We compared those hips with 27 age- and sex-matched adolescents who had CT scans for appendicitis and who had no history of hip pain or symptoms (control group). One orthopaedic surgeon and one pediatric musculoskeletal radiologist, not invoved in the care of the patients included in the study, measured the lateral center-edge angle, acetabular index, acetabular depth/width ratio, acetabular anteversion angle (10 mm from the dome and at the level of the center of the femoral heads), and the anterior and posterior sector angles in the dislocated hip; the contralateral uninvolved hip of the patients with hip dislocations; and both hips in the matched control patients. Both the study and control groups had 25 (93%) males with a mean age of 13 (± 1.7) years. Inter- and intrarater reliability of measurements was assessed with intraclass correlation coefficient (ICC). There was excellent reliability (ICC > 0.90) for the acetabular anteversion angle measured at the center of the femoral head, the acetabular version 10 mm from the dome, and the posterior acetabular sector angle.
Results: The mean acetabular anteversion angle (± SD) was lower in the study group at 10 mm from the acetabular dome (-0.4° ± 9° versus 4° ± 4°; mean difference -5°; 95% confidence interval [CI], -9 to -0.3; p = 0.015) and at the center of the femoral heads (10° ± 5° versus 14° ± 4°; mean difference -3°; 95% CI, -6 to -0.9; p = 0.003). A higher proportion of acetabula was severely retroverted in the study group (14 of 27 [52%]; 95% CI, 33%-71% versus four of 27 [15%]; 95% CI, 1%-28%; p = 0.006). The mean posterior acetabular sector angle was lower in the study group (82° ± 8° versus 90° ± 6°; mean difference -8°; 95% CI, -11 to -4; p < 0.001), whereas no difference was found for the anterior acetabular sector angle (65° ± 6° versus 65° ± 7°; mean difference 0.3°; 95% CI, -3 to 4; p = 0.944). There was no difference for the lateral center-edge angle (27° ± 6° versus 26° ± 5°; p = 0.299), acetabular index (5° ± 3° versus 6 ± 4°; p = 0.761), or acetabular depth/width ration (305 ± 30 versus 304 ± 31; p = 0.944) between groups. Acetabular anteversion angle at the center of the femoral heads (11° ± 4° versus 14° ± 4°; p = 0.006) and the posterior acetabular sector angle (86° ± 7 ° versus 91° ± 6°; p = 0.007) were lower in the contralateral uninvolved hips compared with control hips.
Conclusions: Decreased acetabular anteversion angle and posterior acetabular coverage of the femoral head were associated with posterior dislocation of the hip in adolescents with sports-related injury even in the absence of a high-energy mechanism. Further studies are necessary to clarify whether a causative effect exists between acetabular and femoral morphology and the dislocation of the hip in patients with sports-related injuries.
Level of evidence: Level III, prognostic study.
Conflict of interest statement
Each author certifies that neither he or she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: Acetabular Retroversion and Decreased Posterior Coverage Are Associated With Sports-related Posterior Hip Dislocation in Adolescents.Clin Orthop Relat Res. 2019 May;477(5):1109-1110. doi: 10.1097/CORR.0000000000000581. Clin Orthop Relat Res. 2019. PMID: 30516656 Free PMC article. No abstract available.
Similar articles
-
Femoroacetabular Impingement Is Associated With Sports-Related Posterior Hip Instability in Adolescents: A Matched-Cohort Study.Am J Sports Med. 2016 Sep;44(9):2299-303. doi: 10.1177/0363546516651119. Epub 2016 Jun 16. Am J Sports Med. 2016. PMID: 27311413
-
Morphologic Features of the Contralateral Femur in Patients With Unilateral Slipped Capital Femoral Epiphysis Resembles Mild Slip Deformity: A Matched Cohort Study.Clin Orthop Relat Res. 2018 Apr;476(4):890-899. doi: 10.1007/s11999.0000000000000127. Clin Orthop Relat Res. 2018. PMID: 29481345 Free PMC article.
-
Acetabular Global Insufficiency in Patients with Down Syndrome and Hip-Related Symptoms: A Matched-Cohort Study.J Bone Joint Surg Am. 2017 Oct 18;99(20):1760-1768. doi: 10.2106/JBJS.17.00341. J Bone Joint Surg Am. 2017. PMID: 29040131
-
Hip Dislocation and Subluxation in Athletes: A Systematic Review.Am J Sports Med. 2022 Aug;50(10):2834-2841. doi: 10.1177/03635465211036104. Epub 2021 Oct 8. Am J Sports Med. 2022. PMID: 34623933
-
[Preoperative MR imaging for hip dysplasia : Assessment of associated deformities and intraarticular pathologies].Orthopadie (Heidelb). 2023 Apr;52(4):300-312. doi: 10.1007/s00132-023-04356-8. Epub 2023 Mar 28. Orthopadie (Heidelb). 2023. PMID: 36976331 Free PMC article. Review. German.
Cited by
-
Risk factors and long-term outcomes in anterior iliac and obturator hip dislocation.Eur J Trauma Emerg Surg. 2025 May 17;51(1):205. doi: 10.1007/s00068-025-02885-9. Eur J Trauma Emerg Surg. 2025. PMID: 40380987
-
Acetabular retroversion and cam morphology are contributing risk factors for posterior hip dislocation independent of the trauma mechanism.Arch Orthop Trauma Surg. 2024 Nov;144(11):5013-5020. doi: 10.1007/s00402-024-05595-w. Epub 2024 Sep 28. Arch Orthop Trauma Surg. 2024. PMID: 39340550
-
Is Stage 2 idiopathic osteonecrosis of the hip joint associated with version angles on imaging methods?Jt Dis Relat Surg. 2021;32(3):611-616. doi: 10.52312/jdrs.2021.273. Epub 2021 Nov 19. Jt Dis Relat Surg. 2021. PMID: 34842092 Free PMC article.
-
Anthropometry of the proximal femur and femoral head in children/adolescents using three-dimensional computed tomography-based measurements.Surg Radiol Anat. 2021 Dec;43(12):2009-2023. doi: 10.1007/s00276-021-02841-3. Epub 2021 Oct 1. Surg Radiol Anat. 2021. PMID: 34599355 Free PMC article.
-
Subchondral fatigue fracture of the femoral head in young military recruits: Potential risk factors.World J Clin Cases. 2023 Oct 6;11(28):6733-6743. doi: 10.12998/wjcc.v11.i28.6733. World J Clin Cases. 2023. PMID: 37901035 Free PMC article.
References
-
- Agricola R, Heijboer MP, Ginai AZ, Roels P, Zadpoor AA, Verhaar JA, Weinans H, Waarsing JH. A cam deformity is gradually acquired during skeletal maturation in adolescent and young male soccer players: a prospective study with minimum 2-year follow-up. Am J Sports Med. 2014;42:798-806. - PubMed
-
- Anda S, Terjesen T, Kvistad KA. Computed tomography measurements of the acetabulum in adult dysplastic hips: which level is appropriate? Skeletal Radiol. 1991;20:267-271. - PubMed
-
- Arpey NC, Holte AJ, Tofte JN, Willey MC. Acute periacetabular osteotomy for recurrent posttraumatic dislocation of the hip: a case report. JBJS Case Connect. 2018;8:e39. - PubMed
-
- Berkes MB, Cross MB, Shindle MK, Bedi A, Kelly BT. Traumatic posterior hip instability and femoroacetabular impingement in athletes. Am J Orthop. 2012;41:166-171. - PubMed
-
- Canham CD, Yen YM, Giordano BD. Does Femoroacetabular impingement cause hip instability? A systematic review. Arthroscopy. 2016;32:203-208. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
