Placental Structure in Preterm Birth Among HIV-Positive Versus HIV-Negative Women in Kenya
- PMID: 30272633
- PMCID: PMC6289800
- DOI: 10.1097/QAI.0000000000001871
Placental Structure in Preterm Birth Among HIV-Positive Versus HIV-Negative Women in Kenya
Abstract
Background: Preterm birth (PTB) is a major cause of infant morbidity and mortality in developing countries. Recent data suggest that in addition to Human Immunodeficiency Virus (HIV) infection, use of antiretroviral therapy (ART) increases the risk of PTB. As the mechanisms remain unexplored, we conducted this study to determine whether HIV and ART were associated with placental changes that could contribute to PTB.
Setting: We collected and evaluated placentas from 38 HIV-positive women on ART and 43 HIV-negative women who had preterm deliveries in Nairobi, Kenya.
Methods: Anatomical features of the placentas were examined at gross and microscopic levels. Cases were matched for gestational age and compared by the investigators who were blinded to maternal HIV serostatus.
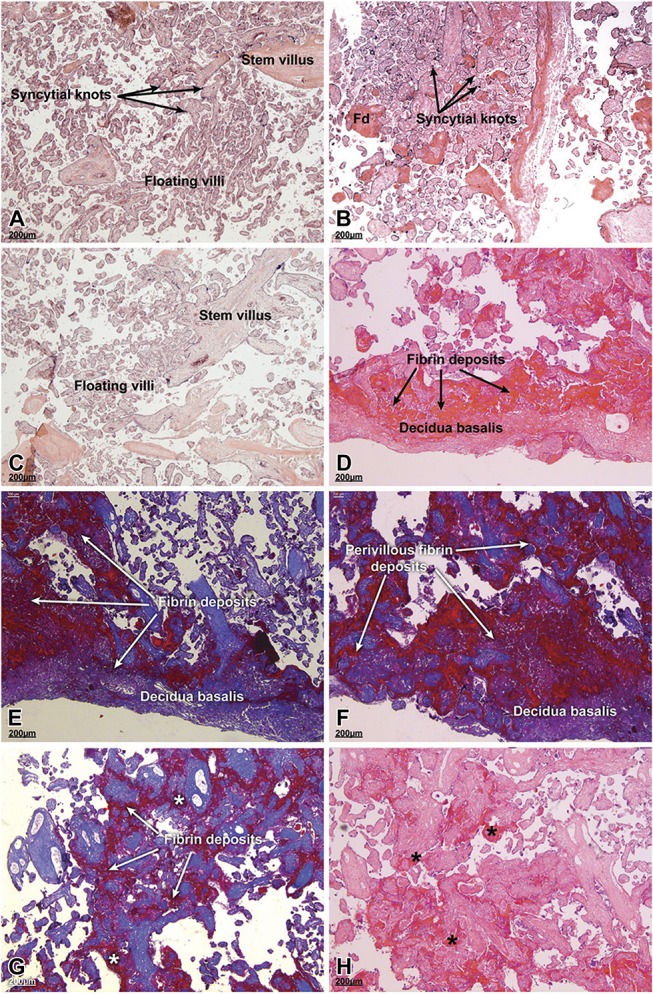
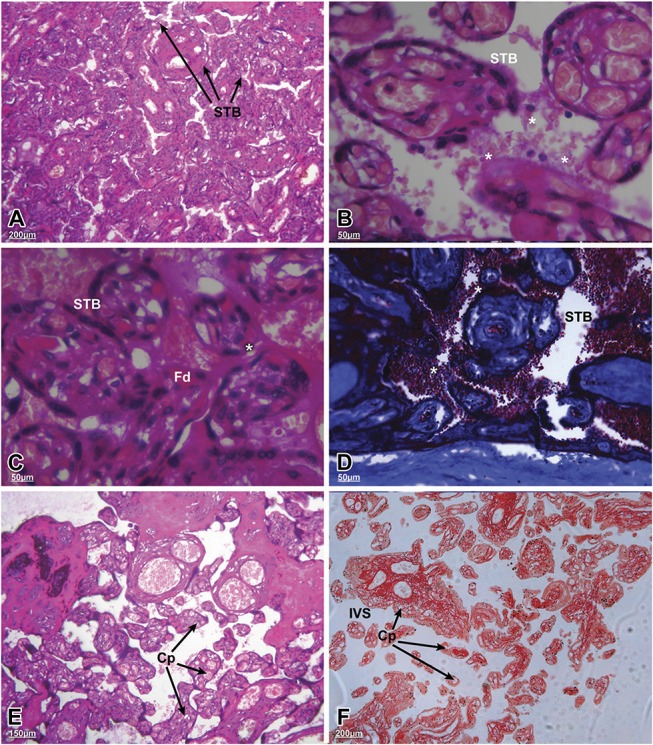
Results: Among preterm placentas, HIV infection was significantly associated with thrombosis (P = 0.001), infarction (P = 0.032), anomalies in cord insertion (P = 0.02), gross evidence of membrane infection (P = 0.043), and reduced placental thickness (P = 0.010). Overall, preterm placentas in both groups were associated with immature villi, syncytial knotting, villitis, and deciduitis. Features of HIV-positive versus HIV-negative placentas included significant fibrinoid deposition with villus degeneration, syncytiotrophoblast delamination, red blood cell adhesion, hypervascularity, and reduction in both surface area and perimeter of the terminal villi.
Conclusions: These results imply that HIV infection and/or ART are associated with morphological changes in preterm placentas that contribute to delivery before 37 weeks. Hypervascularity suggests that the observed pathologies may be attributable, in part, to hypoxia. Further research to explore potential mechanisms will help elucidate the pathways that are involved perhaps pointing to interventions for decreasing the risk of prematurity among HIV-positive women.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures