

18F-fluorocholine positron emission tomography-computed tomography (18F-FCH PET/CT) for staging of high-risk prostate cancer patients
- PMID: 30273114
- PMCID: PMC6456350
- DOI: 10.5489/cuaj.5142
18F-fluorocholine positron emission tomography-computed tomography (18F-FCH PET/CT) for staging of high-risk prostate cancer patients
Abstract
Introduction: We sought to evaluate the diagnostic performance of 18F-fluorocholine positron emission tomography-computed tomography (18F-FCH PET/CT) for initial staging of patients with high-risk prostate cancer. Secondary objectives were to compare the value of 18F-FCH PET/CT to conventional imaging modalities and to evaluate its clinical impact.
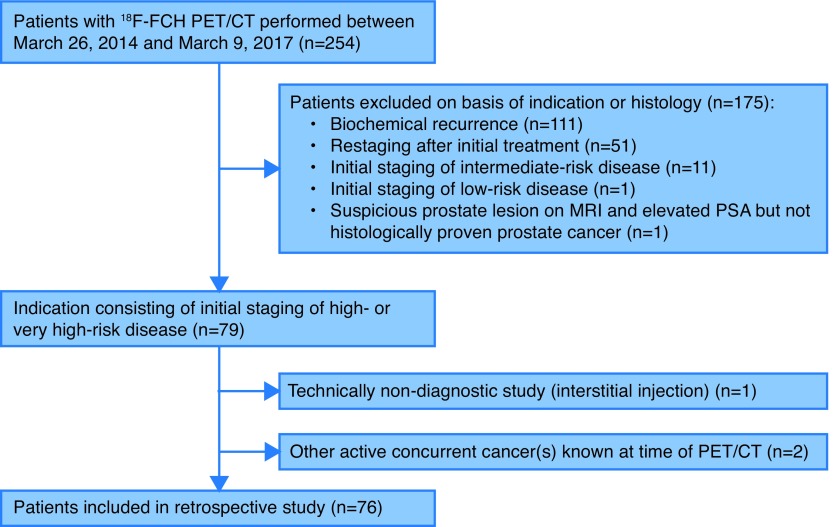
Methods: We conducted a retrospective study of 76 patients who underwent 18F-FCH PET/CT for initial staging of high-risk prostate cancer. Using pre-established validation criteria, sensitivity and specificity were determined for metastatic disease. Results were compared to findings on magnetic resonance imaging (MRI), computed tomography (CT), and bone scan (BS) when available.
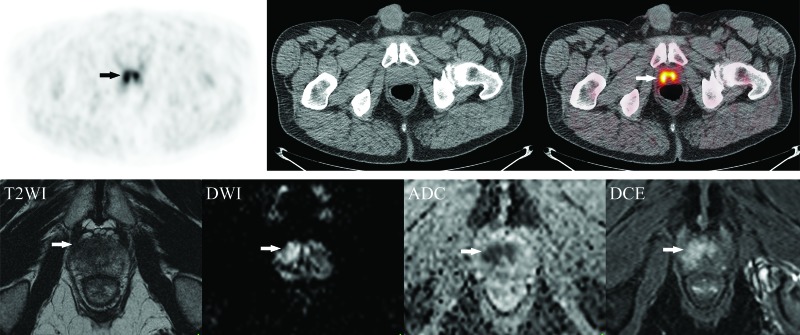
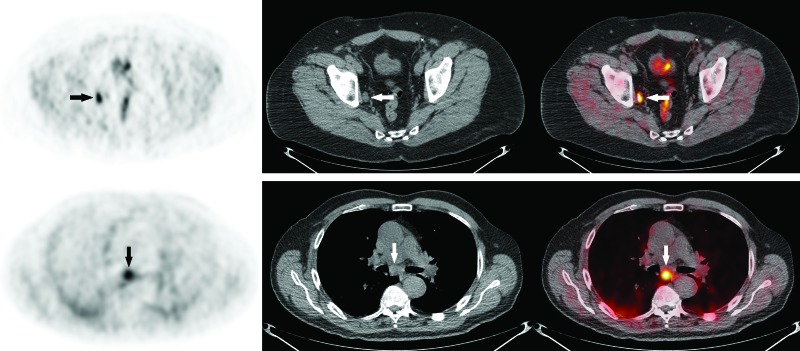
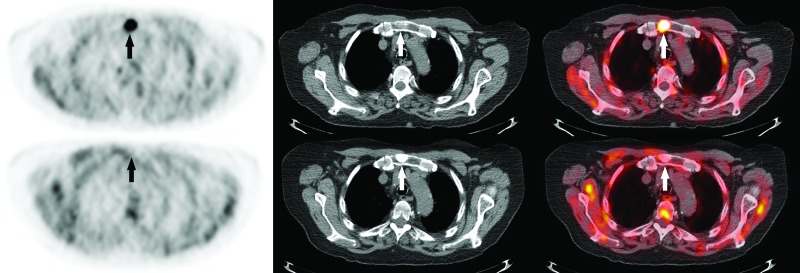
Results: Twenty-two (29%) PET/CT scans were positive, 49 (64%) negative, and five (7%) equivocal for nodal or metastatic disease. Of the positive scans, 17 showed regional lymph node involvement, 12 distant nodes, five bone metastases, and three lung metastases. Overall per-patient sensitivity, specificity, positive and negative predictive values for metastatic disease were 65%, 100%, 100%, and 78%, respectively. Sensitivity, specificity, and positive and negative predictive values were 64%, 100%, 100%, and 80%, respectively, for nodal involvement and 86%, 100%, 100%, and 98%, respectively, for bone and other metastases. Conventional imaging was negative for the lesion(s) found on PET/CT in five patients. PET/CT changed the clinical management in nine patients (12%).
Conclusions: Although 18F-FCH PET/CT offers some benefits over conventional imaging and demonstrates a high specificity, it remains limited by its sensitivity in the context of high-risk prostate cancer staging. PET with novel urea-based small molecule prostate-specific membrane antigen (PSMA) inhibitors may overcome some of these limitations. However, the interpretation of the study result is limited by the lack of available histological gold standard, the inclusion of several patients who received androgen-deprivation therapy (ADT) prior to PET/CT, our retrospective design, and a relatively small sample size.
Conflict of interest statement
Figures
References
-
- Cancer.ca. Canadian Cancer Society’s Advisory Committee on Cancer Statistics. 2017. [Accessed May 19, 2018]. [updated 2017; cited 2018 May 19]. Available at: http://www.cancer.ca/
-
- Sanda MG, Chen RC, Crispino T, et al. 2017. [Accessed Nov 24, 2017]. [cited 2017 November 24]. Available at: http://www.auanet.org/guidelines/clinically-localized-prostate-cancer-ne...
LinkOut - more resources
Full Text Sources
Miscellaneous
