

Klebsiella pneumoniae infection of murine neutrophils impairs their efferocytic clearance by modulating cell death machinery
- PMID: 30273394
- PMCID: PMC6181436
- DOI: 10.1371/journal.ppat.1007338
Klebsiella pneumoniae infection of murine neutrophils impairs their efferocytic clearance by modulating cell death machinery
Abstract
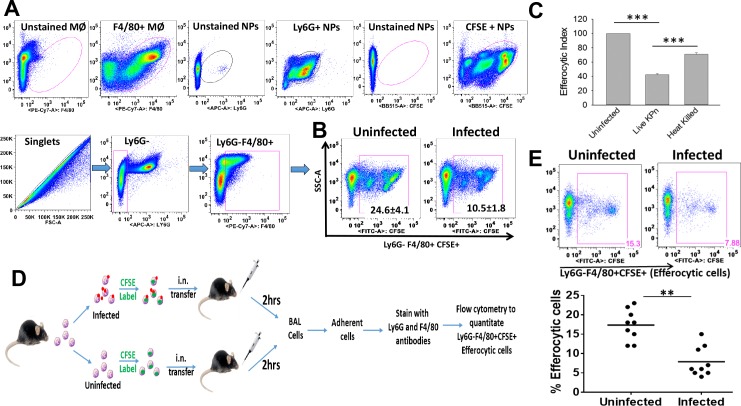
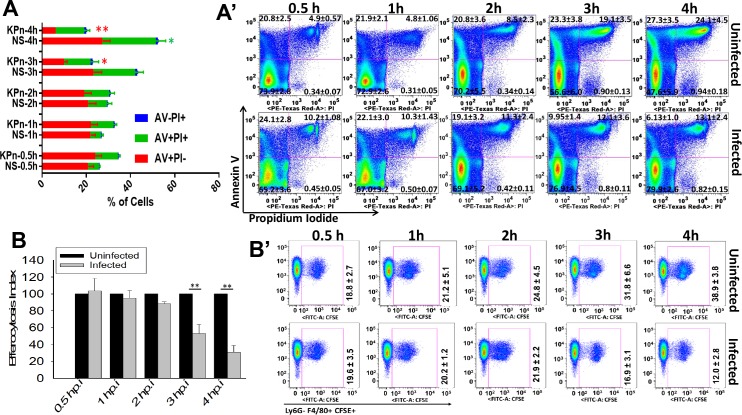
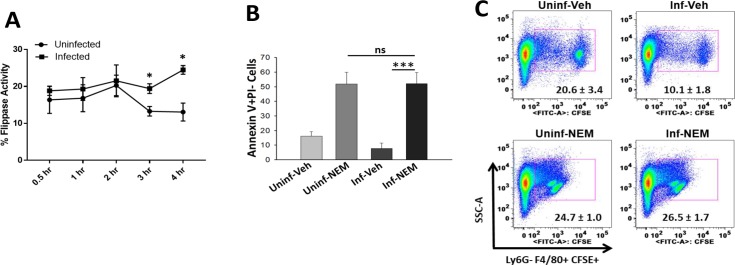
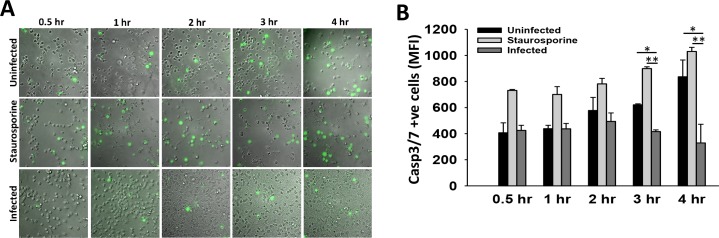
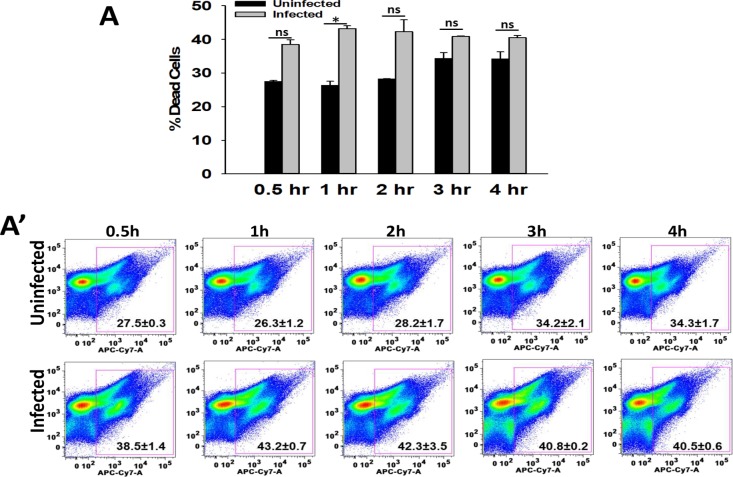
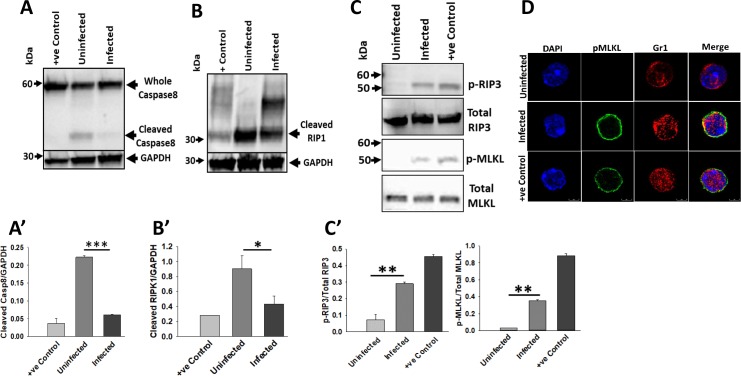
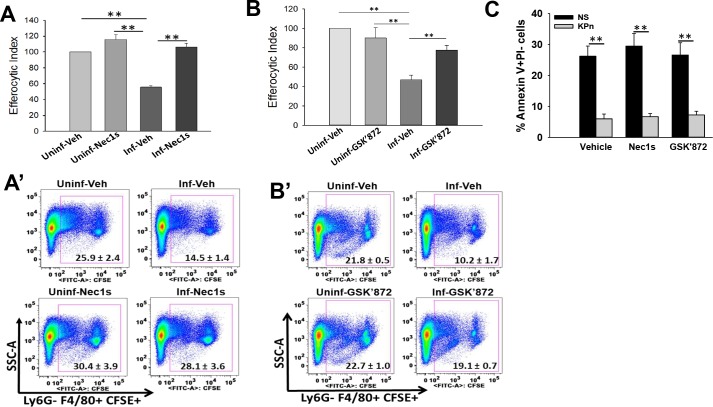
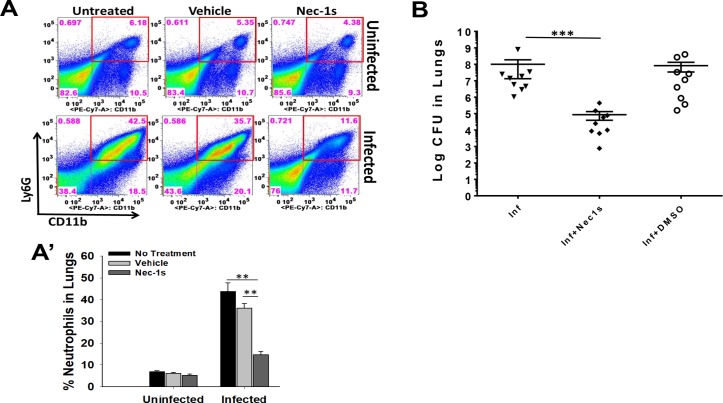
Neutrophils are the first infiltrating cell type essential for combating pneumoseptic infections by bacterial pathogens including Klebsiella pneumoniae (KPn). Following an infection or injury, removal of apoptotic infiltrates via a highly regulated process called efferocytosis is required for restoration of homeostasis, but little is known regarding the effect of bacterial infection on this process. Here we demonstrate that KPn infection impedes the efferocytic uptake of neutrophils in-vitro and in-vivo in lungs by macrophages. This impaired efferocytosis of infected neutrophils coincides with drastic reduction in the neutrophil surface exposure of apoptosis signature phospholipid phosphatidyserine (PS); and increased activity of phospholipid transporter flippases, which maintain PS in the inner leaflet of plasma membrane. Concomitantly, pharmacological inhibition of flippase activity enhanced PS externalization and restored the efferocytosis of KPn infected neutrophils. We further show that KPn infection interferes with apoptosis activation and instead activates non-apoptotic programmed cell death via activation of necroptosis machinery in neutrophils. Accordingly, pharmacological inhibition of necroptosis by RIPK1 and RIPK3 inhibitors restored the efferocytic uptake of KPn infected neutrophils in-vitro. Importantly, treatment of KPn infected mice with necroptosis inhibitor improved the disease outcome in-vivo in preclinical mouse model of KPn pneumonia. To our knowledge, this is the first report of neutrophil efferocytosis impairment by KPn via modulation of cell death pathway, which may provide novel targets for therapeutic intervention of this infection.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Critical care medicine. 2001;29(7):1303–10. Epub 2001/07/11. . - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
