

The Cancer Immunogram as a Framework for Personalized Immunotherapy in Urothelial Cancer
- PMID: 30274701
- PMCID: PMC6697269
- DOI: 10.1016/j.eururo.2018.09.022
The Cancer Immunogram as a Framework for Personalized Immunotherapy in Urothelial Cancer
Abstract
Context: The abysmal outlook of urothelial cancer (UC) has changed with the introduction of immunotherapy. Still, many patients do not respond and distinctive biomarkers are currently lacking. The rise of this novel armamentarium of immunotherapy treatments, in combination with the complex biology of an immunological tumor response, warrants the development of a comprehensive framework that can provide an overview of important immunological processes at play in individual patients.
Objective: To develop a comprehensive framework based on tumor- and host-specific parameters to understand immunotherapy response in UC. This framework can inform rational, biology-driven clinical trials and ultimately guide us toward individualized patient treatment.
Evidence acquisition: A literature review was conducted on UC immunotherapy, clinical trial data, and biomarkers of response to checkpoint inhibition.
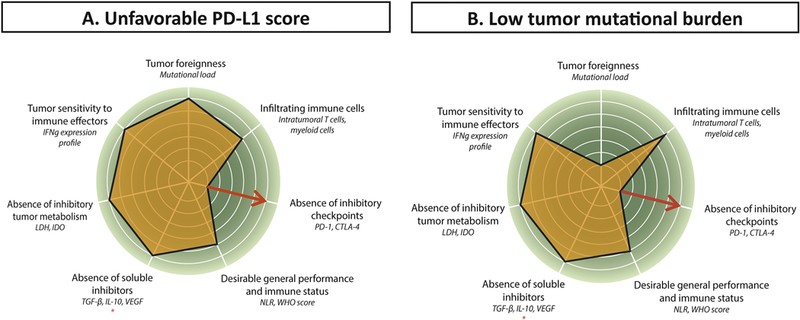
Evidence synthesis: Here, we propose a UC immunogram, based on currently available clinical and translational data. The UC immunogram describes several tumor- and host-specific parameters that are required for successful immunotherapy treatment. These seven parameters are tumor foreignness, immune cell infiltration, absence of inhibitory checkpoints, general performance and immune status, absence of soluble inhibitors, absence of inhibitory tumor metabolism, and tumor sensitivity to immune effectors.
Conclusions: Longitudinal integration of individual patient parameters may ultimately lead to personalized and dynamic immunotherapy, to adjust to the Darwinian forces that drive tumor evolution. Incorporating multiparameter biomarkers into quantitative predictive models will be a key challenge to integrate the immunogram into daily clinical practice.
Patient summary: Here, we propose the urothelial cancer immunogram, a novel way of describing important immunological characteristics of urothelial cancer patients and their tumors. Seven characteristics determine the chance of having an immunological tumor response. Using this immunogram, we aim to better understand why some patients respond to immunotherapy and some do not, to ultimately improve anticancer therapy.
Keywords: Biomarkers; Cytotoxic T lymphocyte–associated protein 4; Immune checkpoint inhibitors; Immunotherapy; Programmed cell death 1; Programmed cell death receptor ligand 1; Urothelial cell cancer.
Copyright © 2018 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures

Comment in
-
The Cancer Immunogram: A Pledge for a Comprehensive Biomarker Approach for Personalized Immunotherapy in Urothelial Cancer.Eur Urol. 2019 Mar;75(3):445-447. doi: 10.1016/j.eururo.2018.12.005. Epub 2018 Dec 15. Eur Urol. 2019. PMID: 30558899 No abstract available.
References
-
- Powles T, Duran I, van der Heijden MS, et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): a multicentre, open-label, phase 3 randomised controlled trial. Lancet 2018;391:748–57. - PubMed
-
- Blank CU, Haanen JB, Ribas A, Schumacher TN. Cancer immunology. The “cancer immunogram”. Science 2016;352:658–60. - PubMed
-
- Karasaki T, Nagayama K, Kuwano H, et al. An immunogram for the cancer-immunity cycle: towards personalized immunotherapy of lung cancer. J Thorac Oncol 2017;12:791–803. - PubMed
-
- Gilboa E The makings of a tumor rejection antigen. Immunity 1999;11:263–70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
