

Primary Whole-gland Cryoablation for Prostate Cancer: Biochemical Failure and Clinical Recurrence at 5.6 Years of Follow-up
- PMID: 30274702
- PMCID: PMC9827755
- DOI: 10.1016/j.eururo.2018.09.004
Primary Whole-gland Cryoablation for Prostate Cancer: Biochemical Failure and Clinical Recurrence at 5.6 Years of Follow-up
Abstract
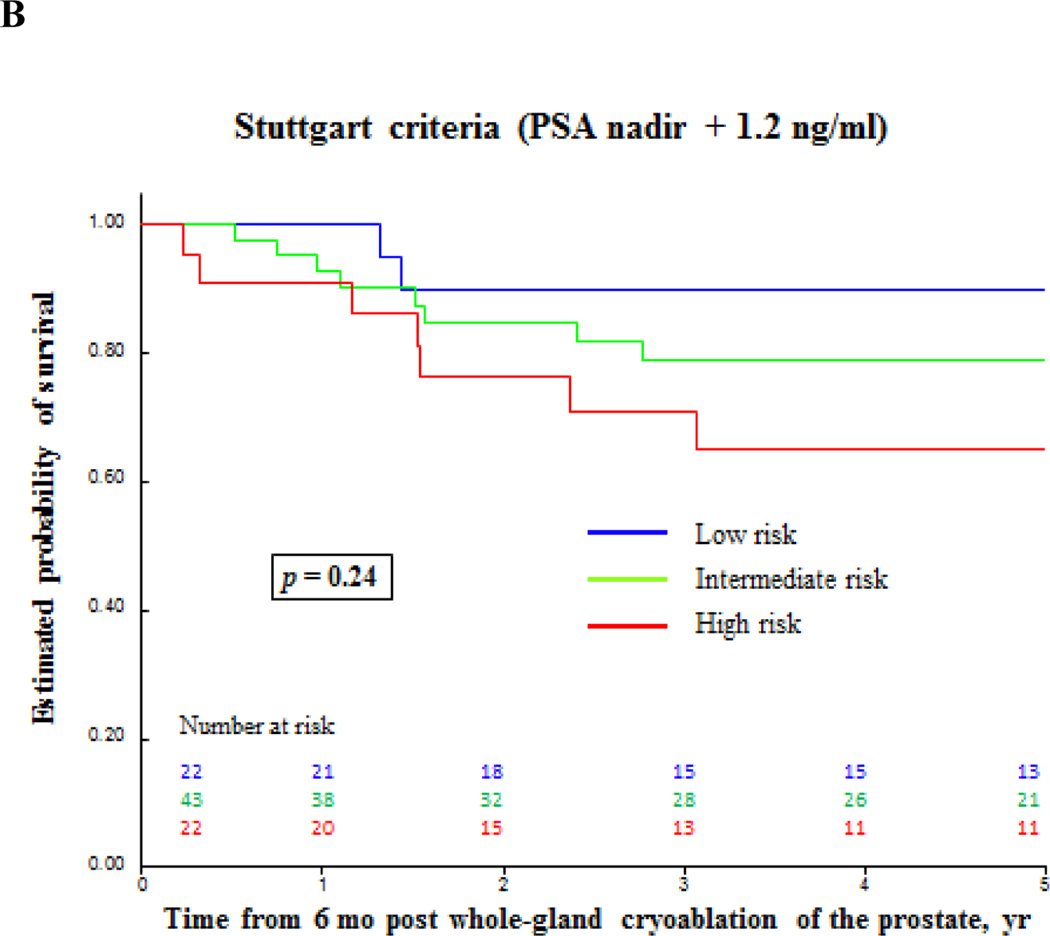
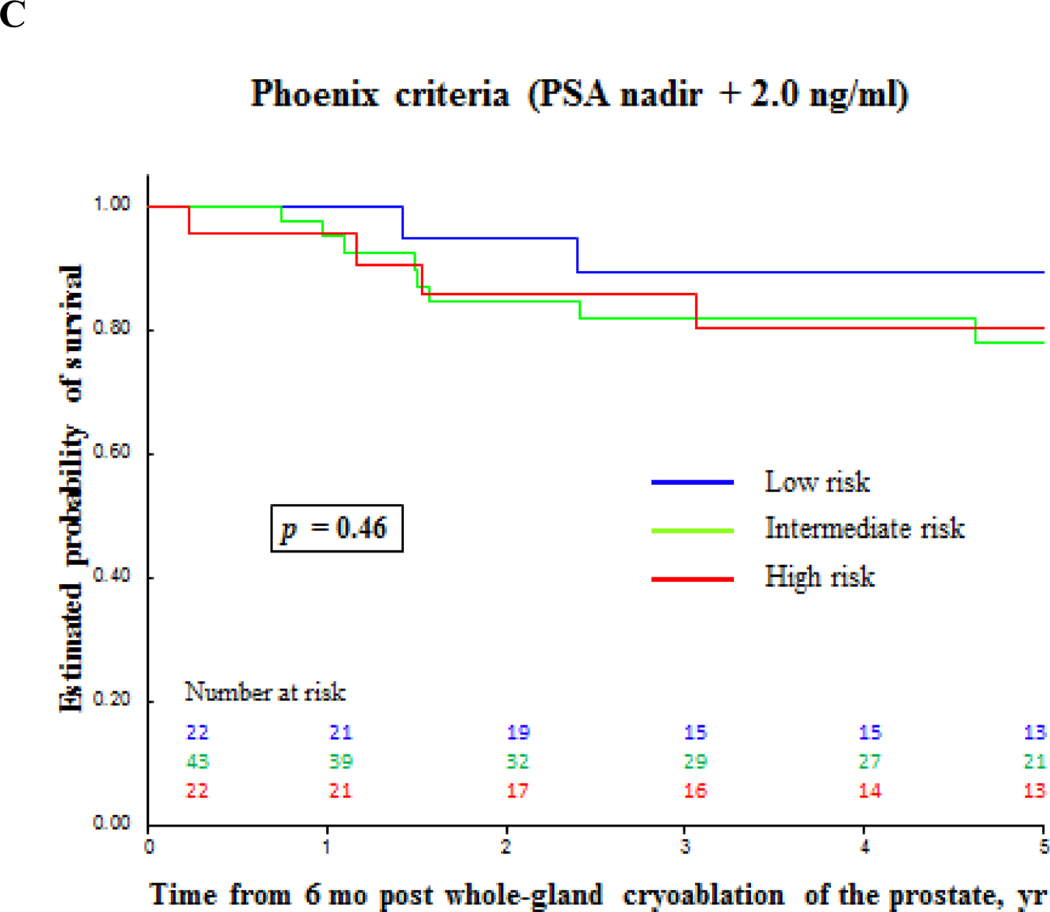
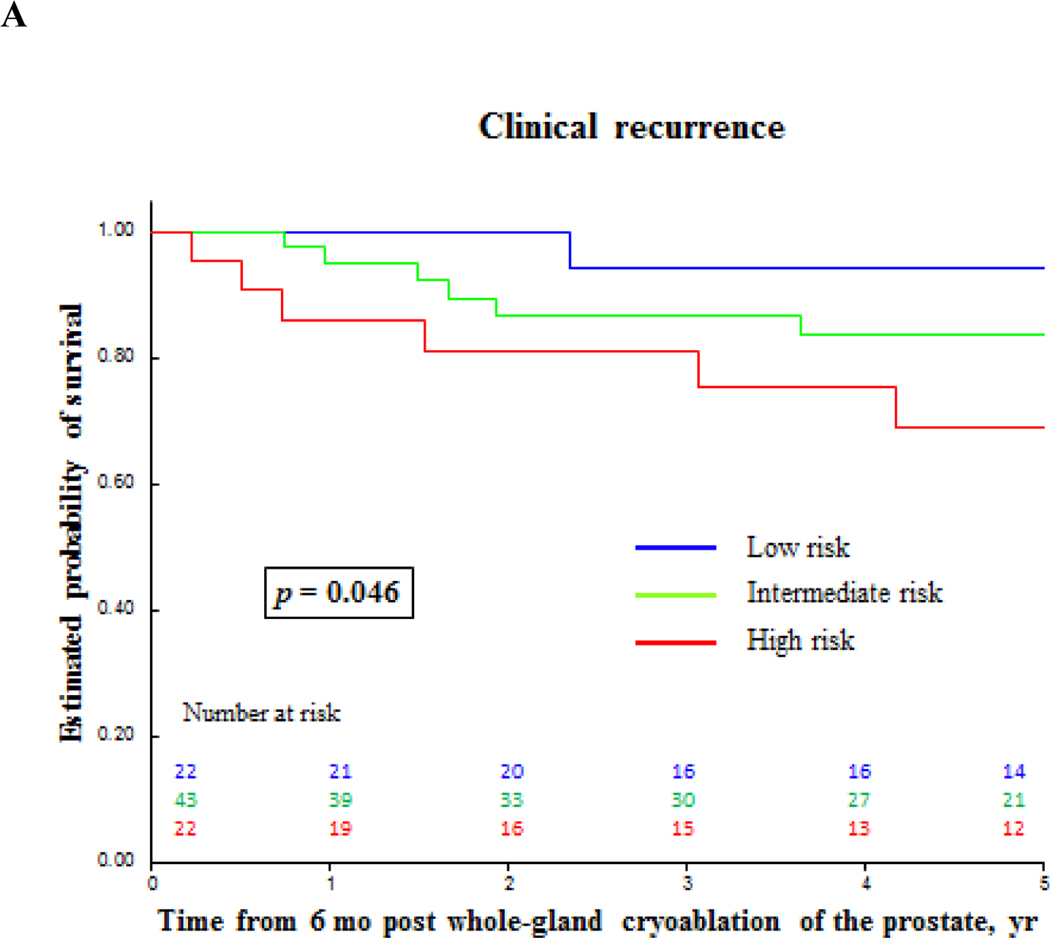
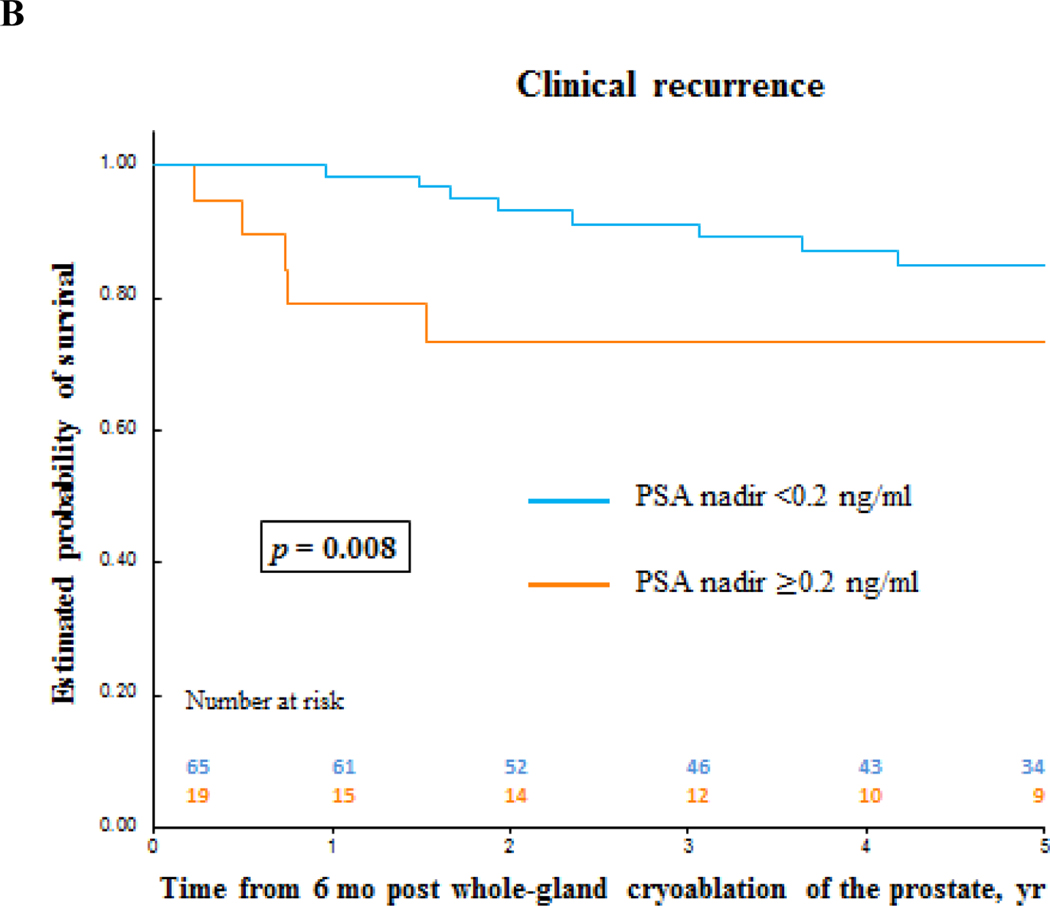
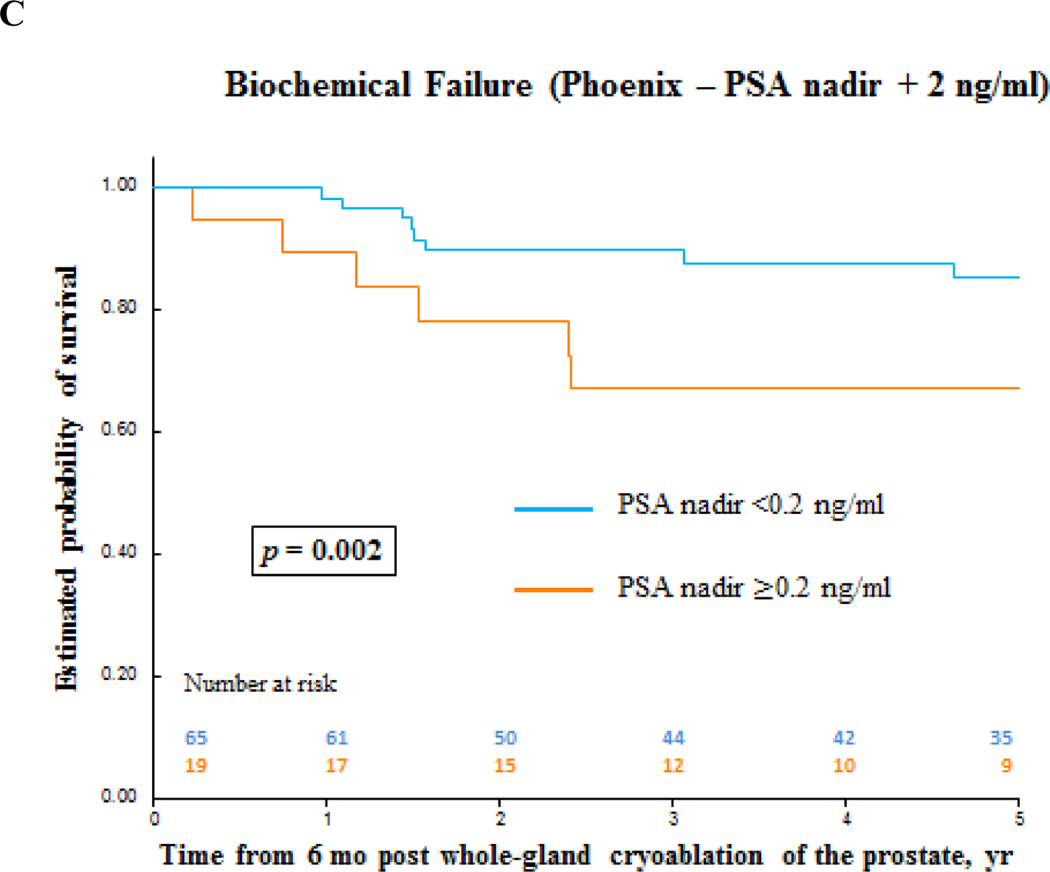
We retrospectively evaluated complications and functional and oncologic outcomes of 94 consecutive men who underwent primary whole-gland cryoablation for localized prostate cancer (PCa) from 2002 to 2012. Kaplan-Meier and multivariable Cox regression analyses were performed using a landmark starting at 6 mo of follow-up. In total, 75% patients had D'Amico intermediate- (48%) or high- (27%) risk PCa. Median follow-up was 5.6 yr. Median time to prostate-specific antigen (PSA) nadir was 3.3 mo, and 70 patients reached PSA <0.2ng/ml postcryoablation. The 90-d high-grade (Clavien Grade IIIa) complication rate was 3%, with no rectal fistulas reported. Continence and potency rates were 96% and 11%, respectively. The 5-yr biochemical failure-free survival (PSA nadir+2ng/ml) was 81% overall and 89% for low-, 78% for intermediate-, and 80% for high-risk PCa (p=0.46). The median follow-up was 5.6 and 5.1 yr for patients without biochemical failure and with biochemical failure, respectively. The 5-yr clinical recurrence-free survival was 83% overall and 94% for low-, 84% for intermediate-, and 69% for high-risk PCa (p=0.046). Failure to reach PSA nadir <0.2ng/ml within 6 mo postcryoablation was an independent predictor for biochemical failure (p=0.006) and clinical recurrence (p=0.03). The 5-yr metastases-free survival was 95%. Main limitation is retrospective evaluation. Primary whole-gland cryoablation for PCa provides acceptable medium-term oncologic outcomes and could be an alternative for radiation therapy or radical prostatectomy. PATIENT SUMMARY: Cryoablation is a safe, minimally-invasive procedure that uses cold temperatures delivered via probes through the skin to kill prostate cancer (PCa) cells. Whole-gland cryoablation may offer an alternative treatment option to surgery and radiotherapy. We found that patients had good cancer outcomes 5 yr after whole-gland cryoablation, and those with a prostate-specific antigen value ≥0.2ng/ml within 6 mo after treatment were more likely to have PCa recurrence.
Keywords: Biochemical failure; Clinical recurrence; Cryoablation; Prostate cancer.
Copyright © 2018 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Hemigland Cryoablation of Localized Low, Intermediate and High Risk Prostate Cancer: Oncologic and Functional Outcomes at 5 Years.J Urol. 2019 Dec;202(6):1188-1198. doi: 10.1097/JU.0000000000000456. Epub 2019 Jul 26. J Urol. 2019. PMID: 31347953 Free PMC article.
-
Oncological and functional outcomes of men undergoing primary whole gland cryoablation of the prostate: A 20-year experience.Cancer. 2022 Nov 1;128(21):3824-3830. doi: 10.1002/cncr.34458. Epub 2022 Sep 15. Cancer. 2022. PMID: 36107496
-
Predictors of prostate-specific antigen biochemical recurrence in patients undergoing primary whole-gland prostate cryoablation.Ann Surg Oncol. 2015 May;22(5):1612-7. doi: 10.1245/s10434-014-3942-9. Epub 2014 Oct 7. Ann Surg Oncol. 2015. PMID: 25287436
-
Salvage cryoablation for locally recurrent prostate cancer following primary radiotherapy.Eur Urol. 2012 Jun;61(6):1204-11. doi: 10.1016/j.eururo.2012.02.051. Epub 2012 Mar 8. Eur Urol. 2012. PMID: 22421081 Review.
-
Local Failure Events in Prostate Cancer Treated with Radiotherapy: A Pooled Analysis of 18 Randomized Trials from the Meta-analysis of Randomized Trials in Cancer of the Prostate Consortium (LEVIATHAN).Eur Urol. 2022 Nov;82(5):487-498. doi: 10.1016/j.eururo.2022.07.011. Epub 2022 Aug 5. Eur Urol. 2022. PMID: 35934601 Review.
Cited by
-
Whole-gland ablation therapy versus active surveillance for low-risk prostate cancer: a prospective study.Cent European J Urol. 2020;73(2):127-133. doi: 10.5173/ceju.2020.0009. Epub 2020 Apr 8. Cent European J Urol. 2020. PMID: 32782830 Free PMC article.
-
Focal therapy for localized prostate cancer in the era of routine multi-parametric MRI.Prostate Cancer Prostatic Dis. 2020 Jun;23(2):232-243. doi: 10.1038/s41391-020-0206-6. Epub 2020 Feb 12. Prostate Cancer Prostatic Dis. 2020. PMID: 32051551 Review.
-
mpMRI-US Fusion-Guided Targeted Cryotherapy in Patients with Primary Localized Prostate Cancer: A Prospective Analysis of Oncological and Functional Outcomes.Cancers (Basel). 2022 Jun 17;14(12):2988. doi: 10.3390/cancers14122988. Cancers (Basel). 2022. PMID: 35740653 Free PMC article.
-
Systematic Review of Focal and Salvage Cryotherapy for Prostate Cancer.Cureus. 2022 Jun 28;14(6):e26400. doi: 10.7759/cureus.26400. eCollection 2022 Jun. Cureus. 2022. PMID: 35911314 Free PMC article. Review.
-
Hemigland Cryoablation of Localized Low, Intermediate and High Risk Prostate Cancer: Oncologic and Functional Outcomes at 5 Years.J Urol. 2019 Dec;202(6):1188-1198. doi: 10.1097/JU.0000000000000456. Epub 2019 Jul 26. J Urol. 2019. PMID: 31347953 Free PMC article.
References
-
- Cornford P, Bellmunt J, Bolla M, et al. EAU-ESTRO-SIOG Guidelines on prostate cancer. Part II: treatment of relapsing, metastatic, and castration-resistant prostate cancer. Eur Urol 2017;71:630–42. - PubMed
-
- Levy DA, Ross AE, ElShafei A, Krishnan N, Hatem A, Jones JS. Definition of biochemical success following primary whole gland prostate cryoablation. J Urol 2014;192:1380–4. - PubMed
-
- Jones JS, Rewcastle JC, Donnelly BJ, Lugnani FM, Pisters LL, Katz AE. Whole gland primary prostate cryoablation: initial results from the cryo on-line data registry. J Urol 2008;180:554–8. - PubMed
-
- Ukimura O, de Castro Abreu AL, Gill IS, Shoji S, Hung AJ, Bahn D. Image visibility of cancer to enhance targeting precision and spatial mapping biopsy for focal therapy of prostate cancer. BJU Int 2013;111:E354–64. - PubMed
-
- de Castro Abreu AL, Bahn D, Leslie S, et al. Salvage focal and salvage total cryoablation for locally recurrent prostate cancer after primary radiation therapy. BJU Int 2013;112:298–307. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
