

Obesity and Endocrine Management of the Patient With Duchenne Muscular Dystrophy
- PMID: 30275248
- PMCID: PMC6460463
- DOI: 10.1542/peds.2018-0333F
Obesity and Endocrine Management of the Patient With Duchenne Muscular Dystrophy
Abstract
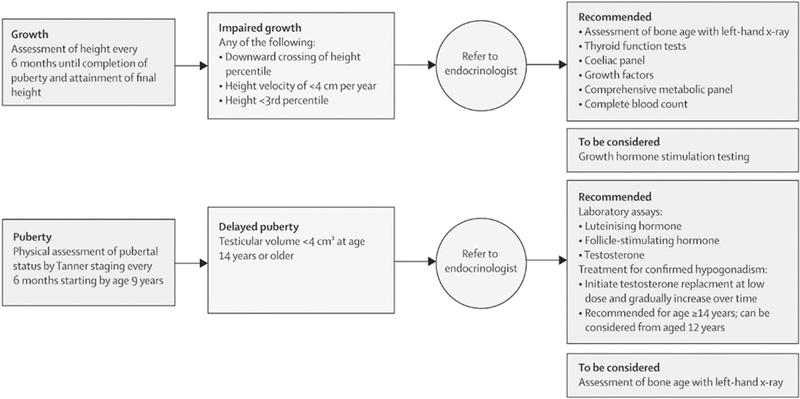
Duchenne muscular dystrophy (DMD) is associated with an increased risk of endocrine complications due to the effects of prolonged glucocorticoid therapy as well as progressive muscle weakness. Categories of complications include obesity and its comorbidities, short stature, pubertal delay, and adrenal insufficiency. Obesity prevention is important for long-term management of patients with DMD. Preventing glucocorticoid-induced weight gain fosters patient mobility, ease of transfer, and reduces sleep-disordered breathing. Metabolic complications from obesity (glucose intolerance, dyslipidemia) also can be avoided. Short stature and pubertal delay may negatively affect self-esteem and peer relationships, and careful monitoring of growth and pubertal development can allow anticipatory counseling. Adrenal insufficiency, a potentially life-threatening complication associated with prolonged glucocorticoid use, must be recognized so as to allow prompt treatment. In this article, we provide a summary of current guidance to ensure comprehensive endocrine management is followed in patients with DMD.
Copyright © 2018 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: Dr Weber has previously served as a paid consultant for Marathon Pharmaceuticals; Drs Ward, Hadjiyannakis, McMillan, and Noritz have indicated they have no potential conflicts of interest to disclose.
Figures
References
-
- Schwartz AV. Diabetes mellitus: does it affect bone? Calcif Tissue Int. 2003;73(6):515–519 - PubMed
-
- Bandini L, Danielson M, Esposito LE, et al. Obesity in children with developmental and/or physical disabilities. Disabil Health J. 2015;8(3):309–316 - PubMed
-
- Vincent C, Gagnon D, Routhier F, et al.; ADMI Group. Service dogs in the province of Quebec: sociodemographic profile of users and the dogs’ impact on functional ability. Disabil Rehabil Assist Technol. 2015;10(2):132–140 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
