

40 Years of Percutaneous Coronary Intervention: History and Future Directions
- PMID: 30275411
- PMCID: PMC6313463
- DOI: 10.3390/jpm8040033
40 Years of Percutaneous Coronary Intervention: History and Future Directions
Abstract
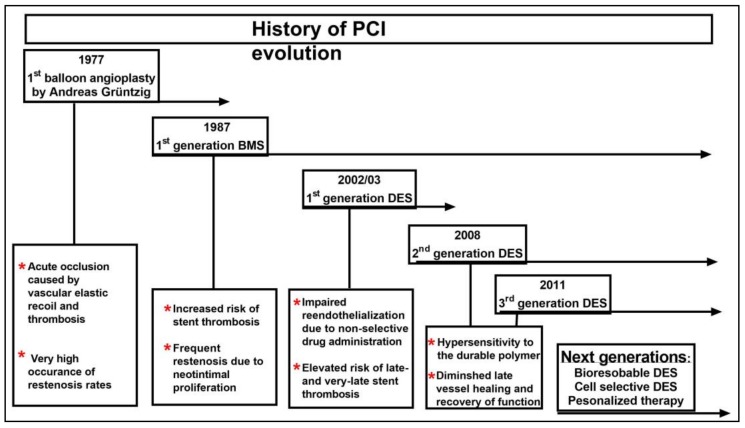
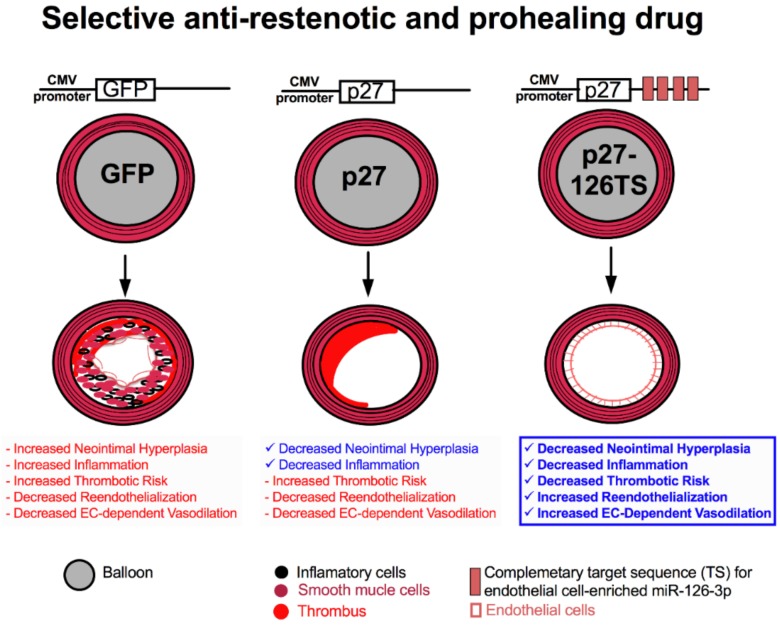
The field of interventional cardiology has evolved significantly since the first percutaneous transluminal coronary angioplasty was performed 40 years ago. This evolution began with a balloon catheter mounted on a fixed wire and has progressed into bare-metal stents (BMS), first-generation drug-eluting stents (DES), second- and third-generation biodegradable polymer-based DES, and culminates with the advent of bioabsorbable stents, which are currently under development. Each step in technological advancement has improved outcomes, while new persisting challenges arise, caused by the stent scaffolds, the polymers employed, and the non-selective cytostatic and cytotoxic drugs eluted from the stents. Despite the promising technological advances made in stent technology, managing the balance between reductions in target lesion revascularization, stent thrombosis, and bleeding remain highly complex issues. This review summarizes the evolution of percutaneous coronary intervention with a focus on vascular dysfunction triggered by the non-selective drugs eluted from various stents. It also provides an overview of the mechanism of action of the drugs currently used in DES. We also discuss the efforts made in developing novel cell-selective drugs capable of inhibiting vascular smooth muscle cell (VSMC) proliferation, migration, and infiltration of inflammatory cells while allowing for complete reendothelialization. Lastly, in the era of precision medicine, considerations of patients' genetic variance associated with myocardial infarction and in-stent restenosis are discussed. The combination of personalized medicine and improved stent platform with cell-selective drugs has the potential to solve the remaining challenges and improve the care of coronary artery disease patients.
Keywords: angioplasty; coronary artery disease; percutaneous intervention; reendothelialization; restenosis; stent.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Benjamin E.J., Blaha M.J., Chiuve S.E., Cushman M., Das S.R., Deo R., de Ferranti S.D., Floyd J., Fornage M., Gillespie C., et al. Heart disease and stroke statistics-2017 update: A report from the American heart association. Circulation. 2017;135:e146–e603. doi: 10.1161/CIR.0000000000000485. - DOI - PMC - PubMed
-
- American Heart Association (AHA) Projections of Cardiovascular Disease Prevalence and Costs: 2015–2035. American Heart Association; Dallas, TX, USA: 2016. pp. 1–54.
-
- Laslett L.J., Alagona P., Jr., Clark B.A., 3rd, Drozda J.P., Jr., Saldivar F., Wilson S.R., Poe C., Hart M. The worldwide environment of cardiovascular disease: Prevalence, diagnosis, therapy, and policy issues: A report from the American college of cardiology. J. Am. Coll. Cardiol. 2012;60:S1–S49. doi: 10.1016/j.jacc.2012.11.002. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
