

Cytogenetics and gene mutations influence survival in older patients with acute myeloid leukemia treated with azacitidine or conventional care
- PMID: 30275526
- PMCID: PMC6286388
- DOI: 10.1038/s41375-018-0257-z
Cytogenetics and gene mutations influence survival in older patients with acute myeloid leukemia treated with azacitidine or conventional care
Abstract
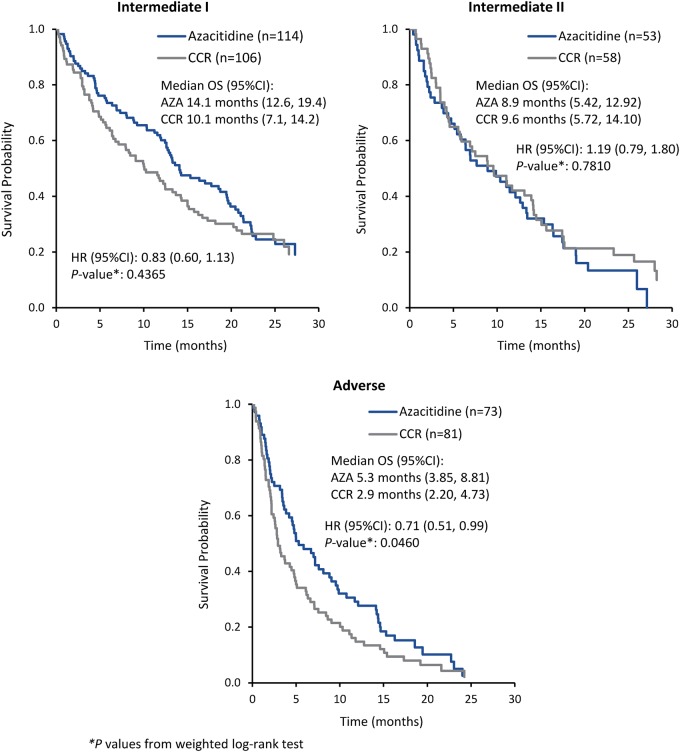
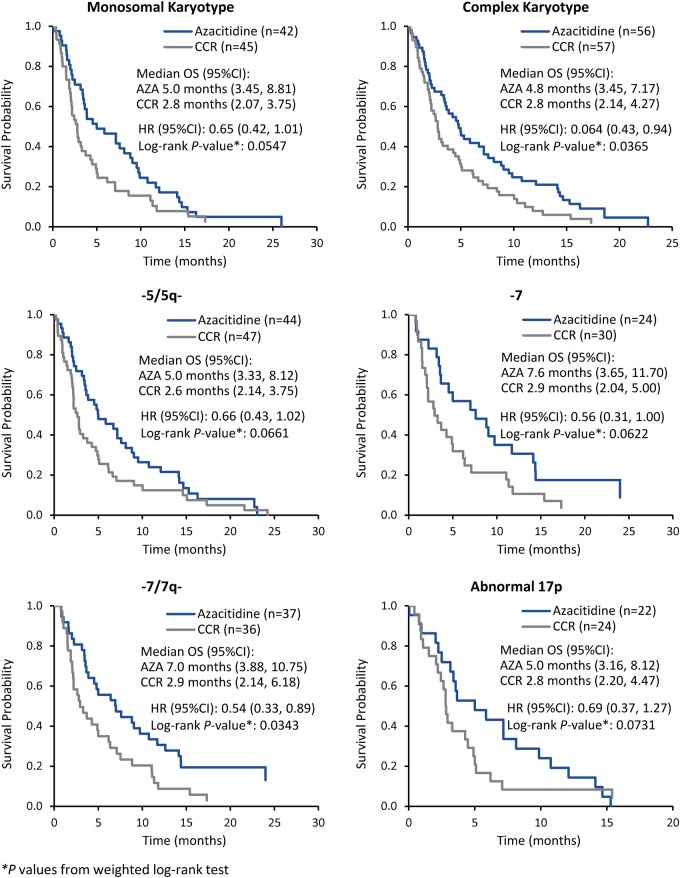
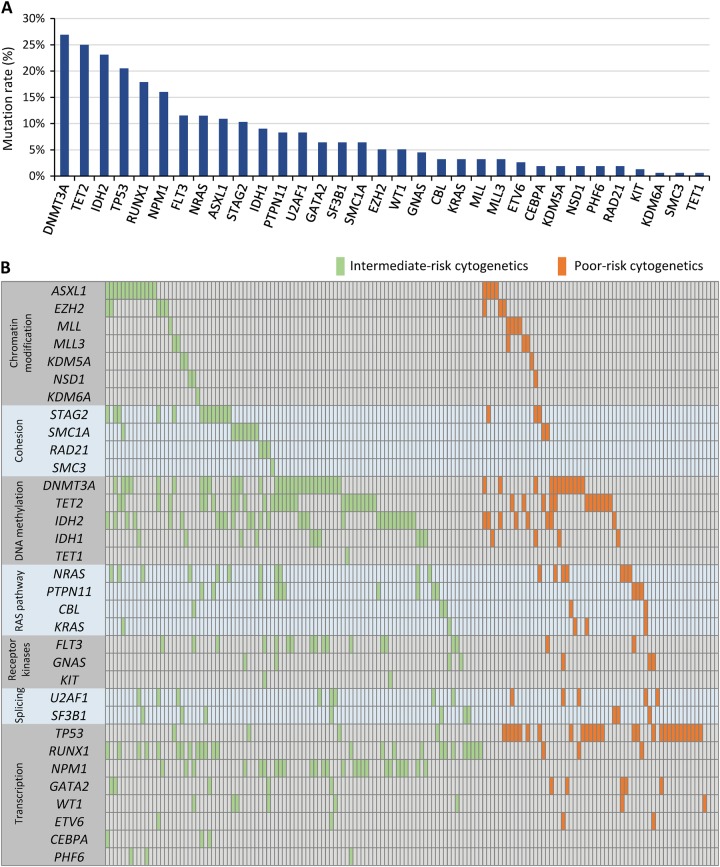
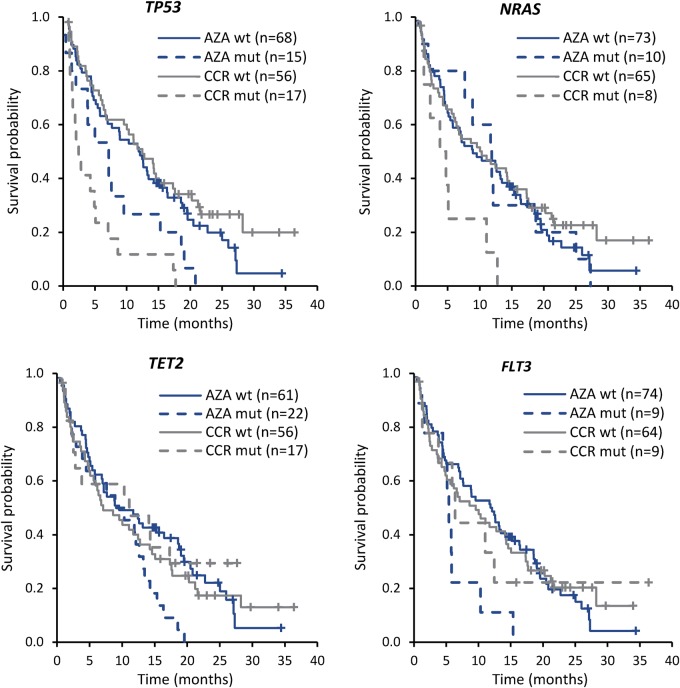
Older patients with newly diagnosed acute myeloid leukemia (AML) in the phase 3 AZA-AML-001 study were evaluated at entry for cytogenetic abnormalities, and a subgroup of patients was assessed for gene mutations. Patients received azacitidine 75 mg/m2/day x7 days (n = 240) or conventional care regimens (CCR; n = 245): intensive chemotherapy, low-dose cytarabine, or best supportive care only. Overall survival (OS) was assessed for patients with common (occurring in ≥10% of patients) cytogenetic abnormalities and karyotypes, and for patients with recurring gene mutations. There was a significant OS improvement with azacitidine vs CCR for patients with European LeukemiaNet-defined Adverse karyotype (HR 0.71 [95%CI 0.51-0.99]; P = 0.046). Azacitidine-treated patients with -5/5q-, -7/7q-, or 17p abnormalities, or with monosomal or complex karyotypes, had a 31-46% reduced risk of death vs CCR. The most frequent gene mutations were DNMT3A (27%), TET2 (25%), IDH2 (23% [R140, 15%; R172, 8%]), and TP53 (21%). Compared with wild-type, OS was significantly reduced among CCR-treated patients with TP53 or NRAS mutations and azacitidine-treated patients with FLT3 or TET2 mutations. Azacitidine may be a preferred treatment for older patients with AML with Adverse-risk cytogenetics, particularly those with chromosome 5, 7, and/or 17 abnormalities and complex or monosomal karyotypes. The influence of gene mutations in azacitidine-treated patients warrants further study.
Conflict of interest statement
H. Döhner: Advisory Boards (with honoraria): AbbVie, Agios, Amgen, Astellas, Astex Pharmaceuticals, Celator, Celgene Corporation, Janssen, Jazz Pharmaceuticals, Novartis, Seattle Genetics, Sunesis. J.F.S.: Advisory Committees, AbbVie, Celgene Corporation, Genentech, Gilead, Janssen, Roche, Takeda; Consultancy, AbbVie, Celgene Corporation, Genentech, Gilead, Janssen, Roche, Takeda; Honoraria, AbbVie, Celgene Corporation, Genentech, Gilead, Janssen, Roche, Takeda; Travel support, AbbVie, Celgene Corporation; Research Funding, AbbVie, Janssen; Speakers Bureau, AbbVie, Celgene Corporation, Gilead, Janssen, Roche. R.M.S.: Consultancy, AbbVie, Agios, Amgen, BristolMeyersSquibb, Celator, Celgene Corporation, Janssen, Juno Therapeutics, Karyopharm, Merck, Novartis, Roche/Genentech, Pfizer, Seattle Genetics, Sunesis Pharmaceuticals, Xenetic Biosciences; Research Funding, Agios, Celator, Karyopharm, Novartis, Pfizer; Advisory Committees, Celgene Corporation. H.K.A.-A.: Consultancy, Honoraria and Research Funding, Celgene; Consultancy, Honoraria and Research Funding, Novartis. V.S.: Consultancy, Amgen, Astex, Celgene Corporation, Janssen, Novartis, Onconova; Honoraria, Celgene Corporation, Janssen, Novartis; Research Funding, Celgene Corporation. P.V.: Honoraria and Research Funding, Celgene Corporation. S.S., C.L.B., L.T., K.J.M., B.S.S.: Employment and equity ownership, Celgene Corporation. L.B.: Advisory Committees BristolMeyersSquibb, Boehringer Ingelheim, Celgene Corporation, Jazz Pharmaceuticals, Novartis, MSD Sharp & Dohme GmbH, Merck, Seattle Genetics. The remaining authors declare that they have no conflict of interest.
Figures

References
-
- Dohner H, Estey EH, Amadori S, Appelbaum FR, Buchner T, Burnett AK, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood. 2010;115:453–74. doi: 10.1182/blood-2009-07-235358. - DOI - PubMed
-
- Grimwade D, Walker H, Oliver F, Wheatley K, Harrison C, Harrison G, et al. The importance of diagnostic cytogenetics on outcome in AML: analysis of 1612 patients entered into the MRC AML 10 trial. The medical research council adult and children’s leukaemia working parties. Blood. 1998;92:2322–33. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
