

Comparison of short-term outcomes between minimally invasive McKeown and Ivor Lewis esophagectomy for esophageal or junctional cancer: a systematic review and meta-analysis
- PMID: 30275710
- PMCID: PMC6157998
- DOI: 10.2147/OTT.S169488
Comparison of short-term outcomes between minimally invasive McKeown and Ivor Lewis esophagectomy for esophageal or junctional cancer: a systematic review and meta-analysis
Abstract
Purpose: Minimally invasive esophagectomy is increasingly performed for esophageal or gastroesophageal junctional cancer, with advantages of improved perioperative outcomes in comparison with open esophagectomy. McKeown and Ivor Lewis are widely used procedures of minimally invasive esophagectomy, and there have been controversies on which one is preferred for patients with resectable esophageal or junctional cancer.
Patients and methods: This review was registered at the International Prospective Register of Systematic Reviews (number CRD42017075989). Studies in PubMed, Embase, Web of Science, the Cochrane Library, and ClinicalTrials.gov were thoroughly investigated. Eligible studies included prospective and retrospective studies evaluating short-term outcomes of minimally invasive McKeown esophagectomy (MIME) vs minimally invasive Ivor Lewis esophagectomy (MILE) in patients with resectable esophageal or junctional tumors. Main parameters included anastomotic leak and 30-day/in-hospital mortality. Overall incidence rates (ORs)/weighted mean difference (WMD) with 95% confidence intervals (CIs) were calculated by employing random-effects models.
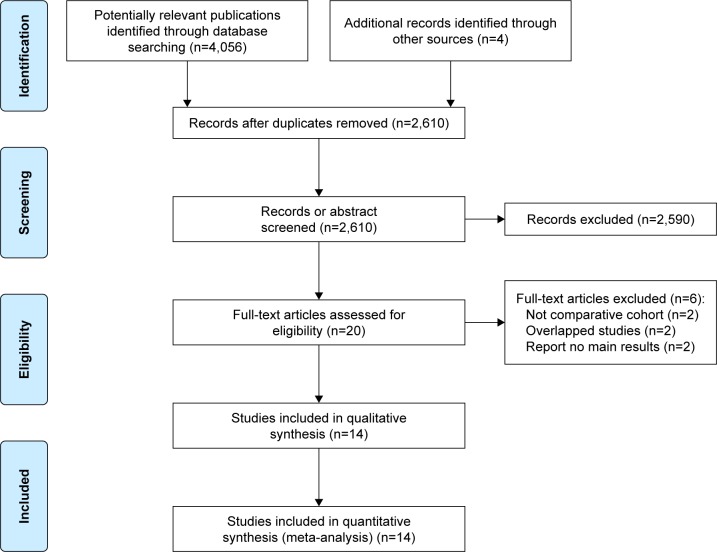
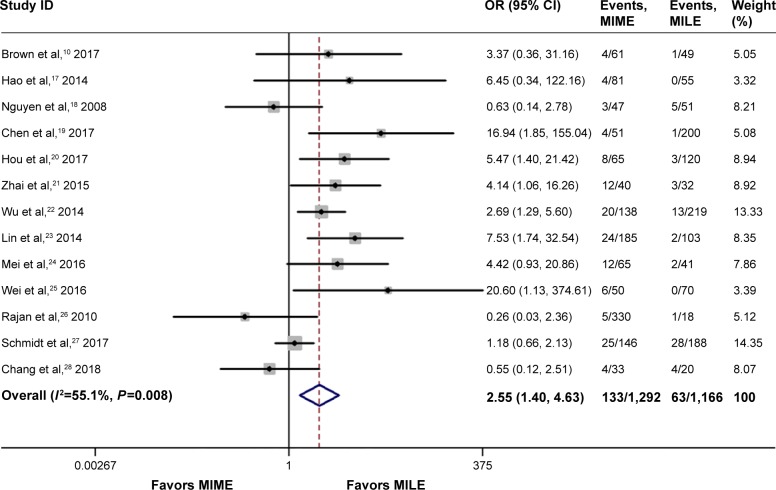
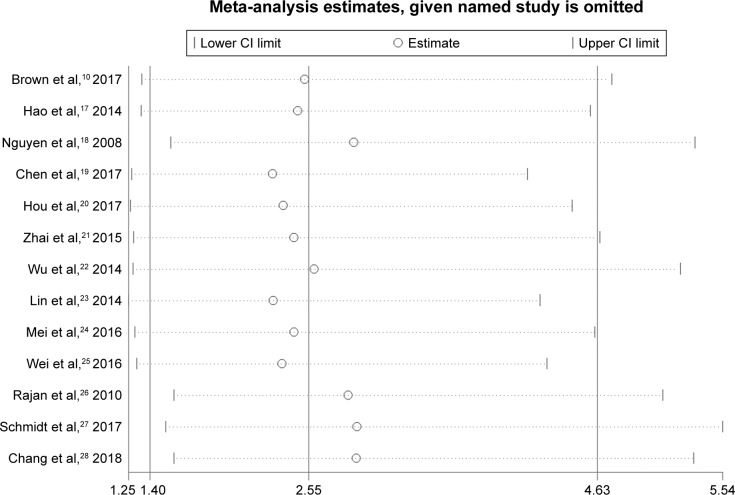
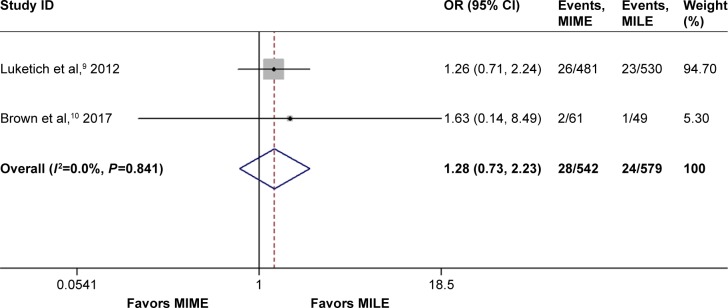
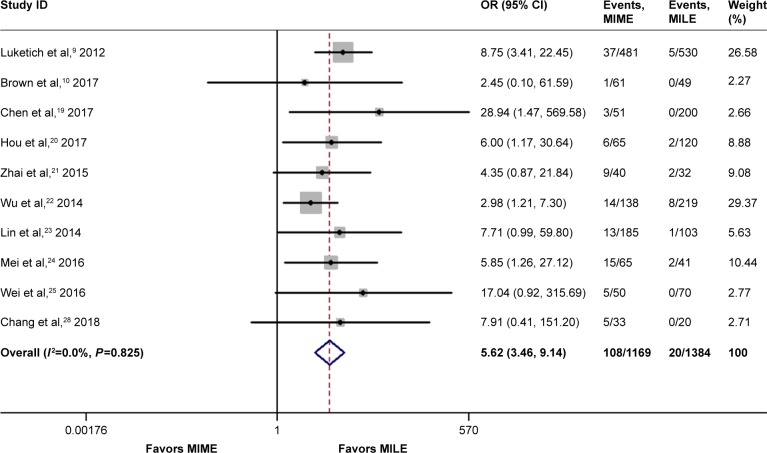
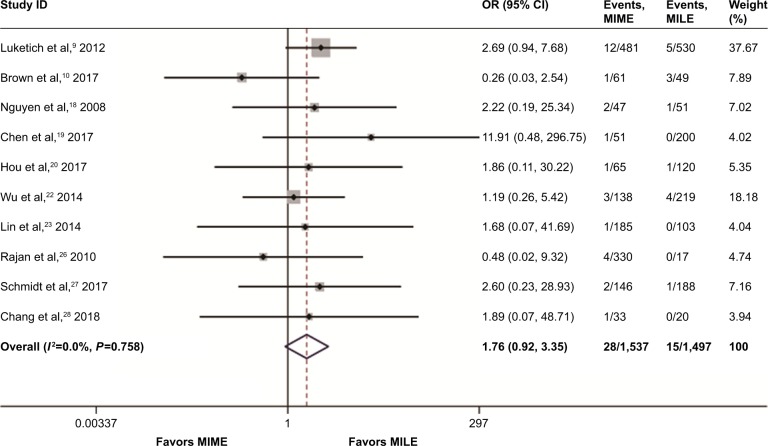
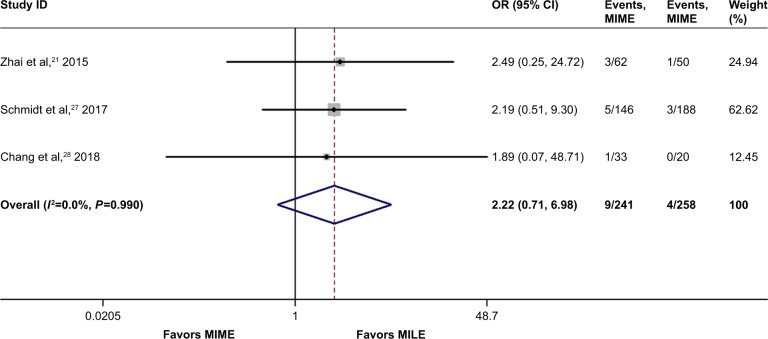
Results: Fourteen studies containing 3,468 cases were included in this meta-analysis. Age, male sex, and American Joint Committee on Cancer (AJCC) stage between the 2 groups were not statistically different. MIME led to more blood loss, longer operating time, and longer hospital stay than MILE. MIME was associated with higher incidence of pulmonary complications (OR =1.96, 95% CI =1.28-3.00) as well as total anastomotic leak (OR =2.55, 95% CI =1.40-4.63), stricture (OR =2.07, 95% CI =1.05-4.07), and vocal cord injury/palsy (OR =5.62, 95% CI =3.46-9.14). In addition, the differences of R0 resection rate, number of lymph modes retrieved, blood transfusion rate, length of intensive care unit stay, incidence of cardiac arrhythmia, and Chyle leak between MIME and MILE were not statistically significant. Notably, incidence of severe anastomotic leak (OR =1.28, 95% CI =0.73-2.24) and 30-day/in-hospital mortality (OR =1.76, 95% CI =0.92-3.36) as well as 90-day mortality (OR =2.22, 95% CI =0.71-6.98) between the 2 procedures were also not significantly different.
Conclusion: This study suggests that MIME and MILE are comparable with respect to clinical safety. MILE may be a better option when oncologically and clinically suitable. MIME is still a safe alternative procedure when clinically indicated. However, this evidence is at risk for bias; randomized controlled trials are needed to validate or correct our results.
Keywords: Ivor Lewis esophagectomy; McKeown esophagectomy; cervical anastomosis; intrathoracic anastomosis; minimally invasive esophagectomy (MIE).
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Similar articles
-
McKeown or Ivor Lewis totally minimally invasive esophagectomy for cancer of the esophagus and gastroesophageal junction: systematic review and meta-analysis.J Thorac Dis. 2017 Jul;9(Suppl 8):S826-S833. doi: 10.21037/jtd.2017.03.173. J Thorac Dis. 2017. PMID: 28815080 Free PMC article.
-
McKeown or Ivor Lewis minimally invasive esophagectomy: a systematic review and meta-analysis.Transl Cancer Res. 2020 Mar;9(3):1518-1527. doi: 10.21037/tcr.2020.01.45. Transl Cancer Res. 2020. PMID: 35117499 Free PMC article.
-
[Short-term efficacy comparison between Ivor-Lewis approach and McKeown approach in minimally invasive esophagectomy].Zhonghua Wei Chang Wai Ke Za Zhi. 2014 Sep;17(9):888-91. Zhonghua Wei Chang Wai Ke Za Zhi. 2014. PMID: 25273657 Chinese.
-
Short-term outcomes of Ivor Lewis vs. McKeown esophagectomy: A meta-analysis.Front Surg. 2022 Oct 28;9:950108. doi: 10.3389/fsurg.2022.950108. eCollection 2022. Front Surg. 2022. PMID: 36386496 Free PMC article. Review.
-
Totally minimally invasive esophagectomy versus hybrid minimally invasive esophagectomy: systematic review and meta-analysis.Dis Esophagus. 2020 Aug 3;33(8):doaa021. doi: 10.1093/dote/doaa021. Dis Esophagus. 2020. PMID: 32350519 Free PMC article.
Cited by
-
Unveiling Therapeutic Targets for Esophageal Cancer: A Comprehensive Review.Curr Oncol. 2023 Oct 30;30(11):9542-9568. doi: 10.3390/curroncol30110691. Curr Oncol. 2023. PMID: 37999111 Free PMC article. Review.
-
Clinical advantage of transmediastinal esophagectomy in terms of postoperative respiratory complications.Int J Clin Oncol. 2023 Jun;28(6):748-755. doi: 10.1007/s10147-023-02328-8. Epub 2023 Mar 16. Int J Clin Oncol. 2023. PMID: 36928515 Review.
-
Safety and efficacy of minimally invasive McKeown esophagectomy in 1023 consecutive esophageal cancer patients: a single-center experience.J Cardiothorac Surg. 2022 Mar 15;17(1):36. doi: 10.1186/s13019-022-01781-2. J Cardiothorac Surg. 2022. PMID: 35292067 Free PMC article.
-
Thirty years of esophageal cancer surgery in Oulu University Hospital.J Thorac Dis. 2021 Aug;13(8):4638-4649. doi: 10.21037/jtd-21-520. J Thorac Dis. 2021. PMID: 34527305 Free PMC article.
-
Minimal invasive versus open esophagectomy for patients with esophageal squamous cell carcinoma after neoadjuvant treatments.BMC Cancer. 2021 Feb 9;21(1):145. doi: 10.1186/s12885-021-07867-9. BMC Cancer. 2021. PMID: 33563244 Free PMC article.
References
-
- Parkin DM, Pisani P, Ferlay J, Statistics GC. Global cancer statistics. CA Cancer J Clin. 1999;49(1):33–64. - PubMed
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. - PubMed
-
- Gupta B, Kumar N. Worldwide incidence, mortality and time trends for cancer of the oesophagus. Eur J Cancer Prev. 2017;26(2):107–118. - PubMed
-
- Stahl M, Budach W, Meyer HJ, Cervantes A, ESMO Guidelines Working Group, Group EGW Esophageal cancer: Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21(Suppl 5):v46–v49. - PubMed
-
- Biere SSAY, van Berge Henegouwen MI, Maas KW, et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. The Lancet. 2012;379(9829):1887–1892. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
