

A NOVEL APPROACH TO TREATMENT UTILIZING BREATHING AND A TOTAL MOTION RELEASE® EXERCISE PROGRAM IN A HIGH SCHOOL CHEERLEADER WITH A DIAGNOSIS OF FROZEN SHOULDER: A CASE REPORT
- PMID: 30276023
- PMCID: PMC6159491
A NOVEL APPROACH TO TREATMENT UTILIZING BREATHING AND A TOTAL MOTION RELEASE® EXERCISE PROGRAM IN A HIGH SCHOOL CHEERLEADER WITH A DIAGNOSIS OF FROZEN SHOULDER: A CASE REPORT
Abstract
Background and purpose: Frozen shoulder (FS) is a condition of the shoulder that is characterized by gradual loss of passive and active range of motion of the glenohumeral joint. Current treatment recommendations remain unclear due to the elusive etiology of FS and absence of nomenclature in the literature. The purpose of this case report is to describe the effects of treatment guided by the assessment and treatment of a breathing pattern disorder (BPD) coupled with Total Motion Release® on a 17-year high school cheerleader with a diagnosis of frozen shoulder.
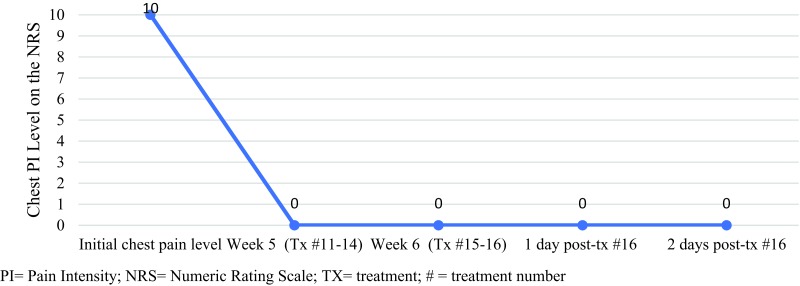
Case description: A 17-year-old female cheerleader reported left anterolateral chest pain after running during cheer practice. The subject continued to experience additional episodes of chest pain and sought out medical care at an emergency department where she was diagnosed with a FS. Clinical findings upon examination included soft tissue muscular irritability, glenohumeral internal and external rotation active range of motion (AROM) loss, and a dysfunctional breathing pattern. Intervention consisted of two types of breathing interventions and a Total Motion Release® (TMR) exercise program. The Numeric Rating Scale (NRS), inclinometer measurements to measure AROM, and breathing assessment outcomes were used to identify patient-reported outcomes and determine treatment effects.
Outcomes: The use of the coupled treatment resulted in a resolution of the patient's primary complaint, an increase in AROM, and an improvement in breathing assessment outcomes. After the first treatment, internal rotation (IR) improved by 27° exceeding a minimal detectable change (MDC) of 8°, and after the second treatment, external rotation (ER) improved by 21° exceeding a MDC of 9°. Equally important, there were improvements in flexion (11°) and abduction (45°) exceeding the MDC of 8° and 4° respectively over the course of treatment. The minimal clinically important difference (MCID) on the NRS was exceeded when the patient returned to activity.
Discussion: In this case report, breathing treatments, coupled with a TMR® exercise program, were beneficial treatments for this patient and provided a clinically meaningful resolution of her condition. Clinicians treating patients who display a similar presentation of frozen shoulder can consider this a possible treatment option.
Levels of evidence: Level 4; single case report.
Keywords: Adhesive capsulitis; breathing pattern disorder; manual therapy.
Figures











References
-
- Griggs SM Ahn A Green A. Idiopathic adhesive capsulitis. J Bone Joint Surg Am. 2000;82(10):1398‐1398. - PubMed
-
- Hannafin JA Chiaia T. Adhesive capsulitis: A treatment approach. Clin Orthop Relat Res. 2000; 372:95‐109. - PubMed
-
- Kelley MJ McClure PW Leggin BG. Frozen shoulder: evidence and a proposed model guiding rehabilitation. J Orthop Sports Phys Ther. 2009;39(2):135‐148 - PubMed
-
- Neviaser JS. Adhesive capsulitis of the shoulder: a study of the pathological findings in periarthritis of the shoulder. J Bone Joint Surg. 1945; 27(2):211‐222.
LinkOut - more resources
Full Text Sources
Research Materials