

T1 Slope Minus Cervical Lordosis (TS-CL), the Cervical Answer to PI-LL, Defines Cervical Sagittal Deformity in Patients Undergoing Thoracolumbar Osteotomy
- PMID: 30276093
- PMCID: PMC6159736
- DOI: 10.14444/5042
T1 Slope Minus Cervical Lordosis (TS-CL), the Cervical Answer to PI-LL, Defines Cervical Sagittal Deformity in Patients Undergoing Thoracolumbar Osteotomy
Abstract
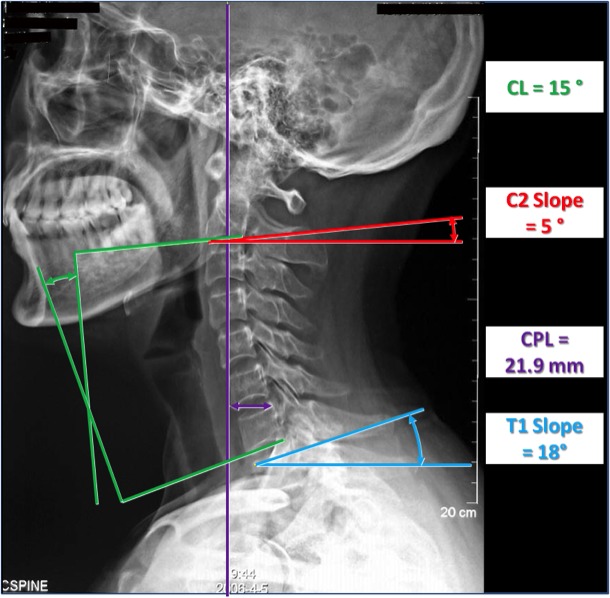
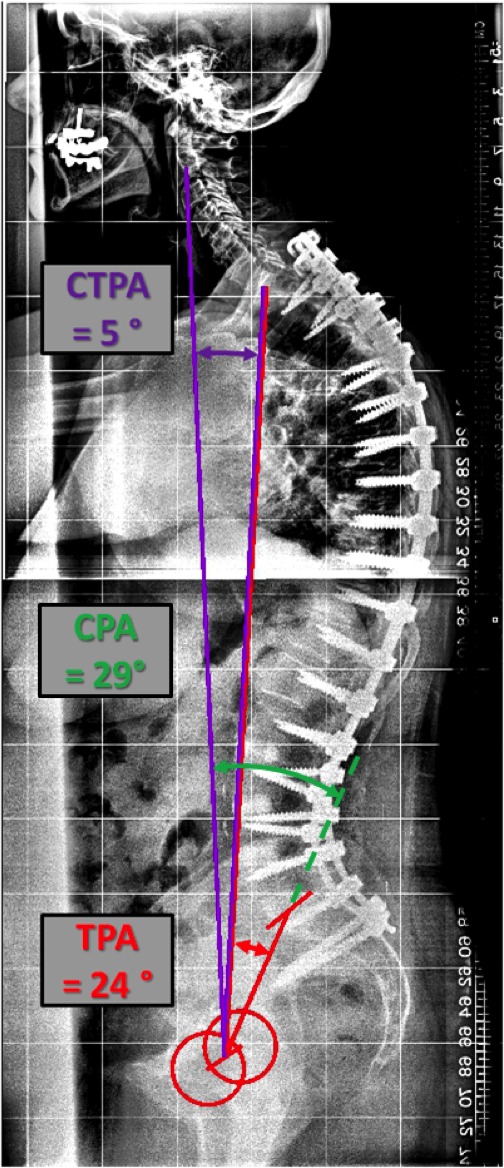
Background: Cervical kyphosis and C2-C7 plumb line (CPL) are established descriptors of cervical sagittal deformity (CSD). Reciprocal changes in these parameters have been demonstrated in thoracolumbar deformity correction. The purpose of this study was to investigate the development of CSD, using T1 slope minus cervical lordosis (TS-CL) to define CSD and to correlate TS-CL and a novel global sagittal parameter, cervical-thoracic pelvic angle (CTPA), with CPL.
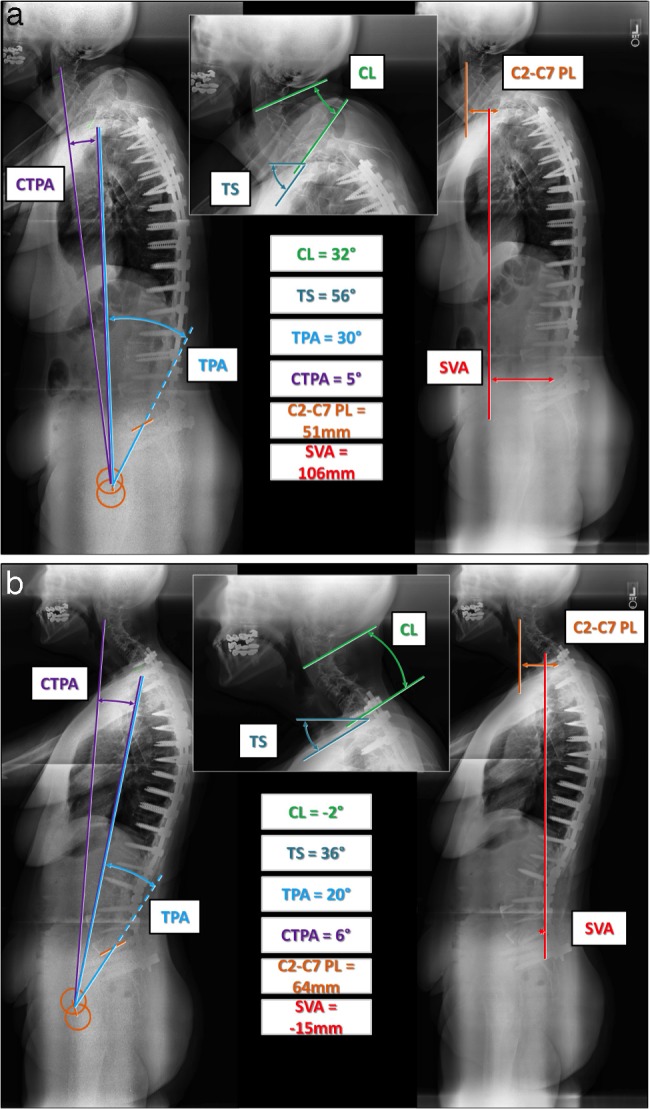
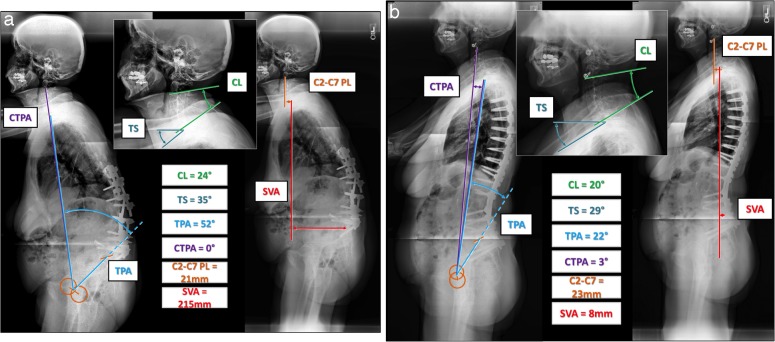
Methods: A multicenter, retrospective analysis of patients with thoracolumbar deformity undergoing three-column osteotomy was performed. Preoperative and postoperative cervical parameters were investigated. Linear regression for postoperative values resulted in a CPL of 4 cm corresponding to a TS-CL threshold of 17°. Patients were classified based on postoperative TS-CL into uncompensated (TS-CL > 17°) or compensated cohorts (TS-CL < 17°); the two were compared using an unpaired t test. Logistic regression modeling was used to determine predictors of postoperative CSD.
Results: A total of 223 patients with thoracolumbar deformity (mean age, 57.56 years) were identified. CTPA correlated with CPL (preoperative r = .85, postoperative r = .69). TS-CL correlated with CTPA (preoperative r = .52, postoperative r = .37) and CPL (preoperative r = .52; postoperative r = .37). CSD had greater preoperative CPL (P < .001) and CTPA (P < .001). The compensated cohort had a decrease in TS-CL (from 10.2 to 8.0) with sagittal vertical axis (SVA) correction, whereas the uncompensated had an increase in TS-CL (from 22.3 to 26.8) with all P < .001. Reciprocal change was demonstrated in the compensated group given that CL decreased with SVA correction (r = .39), but there was no such correlation in the uncompensated. Positive predictors of postoperative CSD included baseline TS-CL > 17° (P = .007), longer fusion (P = .033), and baseline CTPA (P = .029).
Conclusions: TS-CL and CTPA correlated significantly with established sagittal balance measures. Whereas reciprocal change in cervical and thoracolumbar alignment was demonstrated in the compensated cohort, the uncompensated population had progression of their cervical deformities after three-column osteotomy.
Clinical relevance: The balance between TS-CL mirrors the relationship between pelvic incidence minus lumbar lordosis in defining deformities of their respective spinal regions.
Keywords: CPL; TS-CL; alignment; cervical kyphosis; thoracolumbar deformity.
Figures

References
-
- Blondel BS, Schwab F, Ames CP, et al. Podium presented at 19th International Meeting on Advanced Spine Techniques; July 18–21. Istanbul, Turkey: 2012. The crucial role of cervical alignment in regulating sagittal spino-pelvic alignment in human standing posture.
-
- Berthonnaud E, Dimnet J, Roussouly P, Labelle H. Analysis of the sagittal balance of the spine and pelvis using shape and orientation parameters. J Spinal Disord Tech. 2005;18(1):40–47. - PubMed
-
- Lafage V, Schwab F, Skalli W, et al. Standing balance and sagittal plane spinal deformity: analysis of spinopelvic and gravity line parameters. Spine (Phila Pa 1976) 2008;33(14):1572–1578. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous