

Long-Term Experience With Reduction Technique in High-Grade Spondylolisthesis in the Young
- PMID: 30276098
- PMCID: PMC6159655
- DOI: 10.14444/5047
Long-Term Experience With Reduction Technique in High-Grade Spondylolisthesis in the Young
Abstract
Background: Surgical management of high-grade spondylolisthesis in the young is not only challenging but also controversial, from in-situ fusion to complete reduction. It is fraught with dangers such as neurological injury, pseudoarthrosis, and progressive deformity with subsequent global sagittal imbalance. We describe our experience of progressive reduction technique and restoration of lumbosacral alignment.
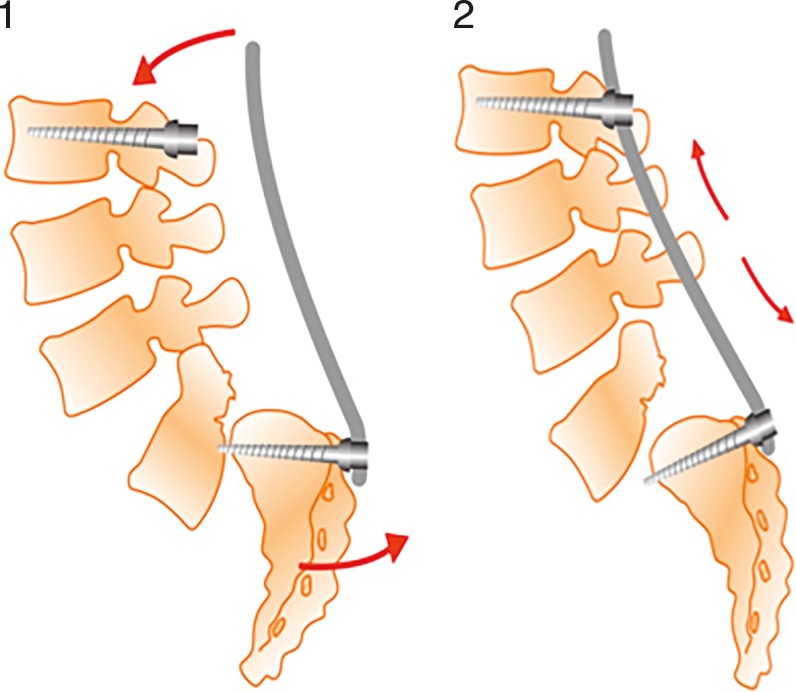
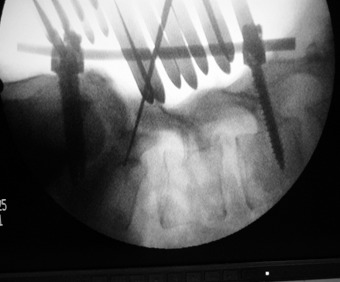
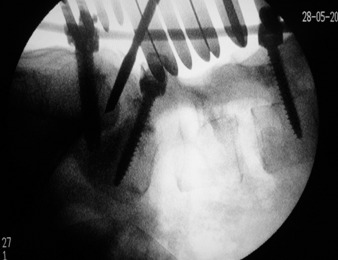
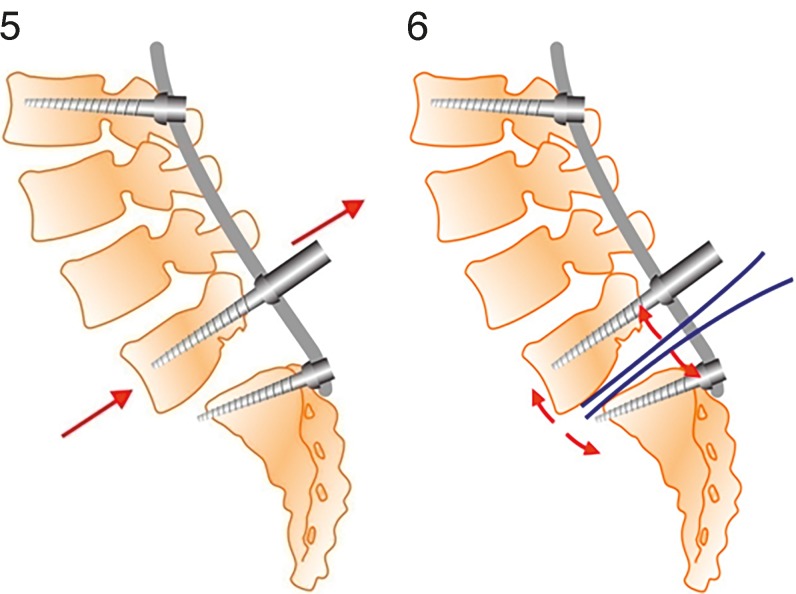
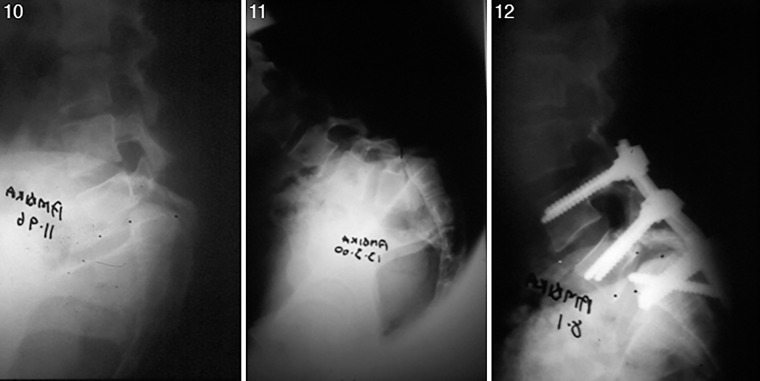
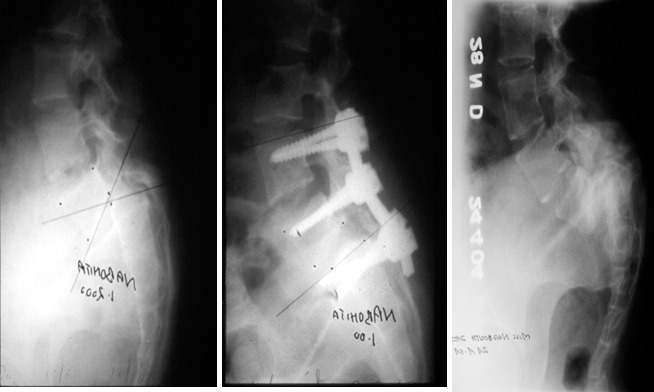
Methods: This study is a retrospective review of patients who underwent surgery between 1998 and 2012. The surgical technique involved positioning the hips in extension with traction, pedicle screw fixation, correction of lumbosacral kyphosis with a specific distraction maneuver, wide decompression, and gradual reduction of the deformity and maintenance of reduction with interbody fusion. All patients were serially assessed at 1, 3, and 6 months and yearly thereafter with clinical, radiological, and Oswestry Disability Index and Visual Analogue Scale outcome measures.
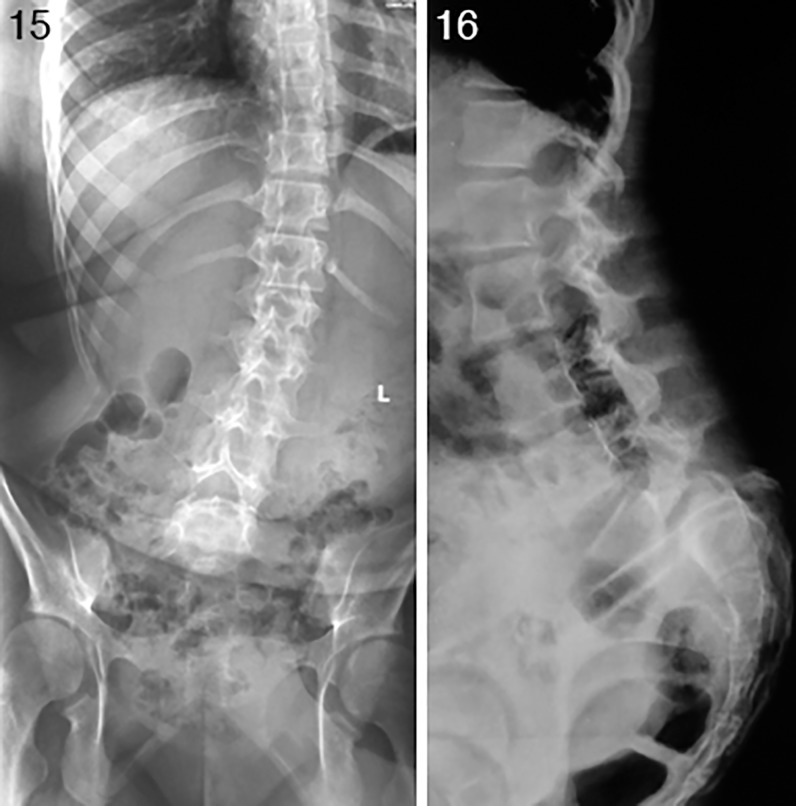
Results: Twenty-seven patients with high-grade spondylolisthesis at L5-S1 (3 cases grade 3, 7 grade 4, 17 grade 5) with an average age of 13.9 years were reviewed. Mean follow-up was 120 months (range 24-192). All patients presented a solid fusion at the 6-month visit; mean slip percentage was reduced from 89% to 23%, with all cases reduced to grade 2 or less. The slip angle improved from 45° to 3° postoperatively, with improvement in sacral slope from 13° to 35°. Four spondyloptosis patients had concomitant scoliosis which corrected spontaneously after the surgery and did not need further intervention. All but one patient (96.2%) had good functional outcomes and returned to their full normal activities. One patient developed a deep infection necessitating implant removal, with eventual deformity progression leading to a poor outcome. Three patients (11.1%) suffered partial drop foot that resolved in full by 12 weeks.
Conclusion: Our technique demonstrated a significant reduction of high grade spondylolisthesis, with restoration of global sagittal balance via correction of the lumbosacral kyphosis. Though surgically demanding, it is safe and reproducible.
Level of evidence: IV.
Keywords: high-grade spondylolisthesis; instrumentation; lumbosacral kyphosis; reduction; sagittal balance.
Conflict of interest statement
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest. The Institutional Review Board of the Apollo Hospital Education and Research Foundation approved this study.
Figures




Similar articles
-
Surgical treatment of high-grade spondylolisthesis: Technique and results.J Orthop. 2020 Aug 25;22:383-389. doi: 10.1016/j.jor.2020.08.015. eCollection 2020 Nov-Dec. J Orthop. 2020. PMID: 32952331 Free PMC article. Review.
-
Transvertebral Transsacral strut grafting for high-grade isthmic spondylolisthesis L5-S1 with fibular allograft.J Spinal Disord Tech. 2008 Jul;21(5):328-33. doi: 10.1097/BSD.0b013e318149e7ea. J Spinal Disord Tech. 2008. PMID: 18600142
-
Posterior lumbar interbody fusion for lytic spondylolisthesis: restoration of sagittal balance using insert-and-rotate interbody spacers.Spine J. 2005 Mar-Apr;5(2):161-9. doi: 10.1016/j.spinee.2004.05.256. Spine J. 2005. PMID: 15749616 Clinical Trial.
-
Partial lumbosacral kyphosis reduction, decompression, and posterior lumbosacral transfixation in high-grade isthmic spondylolisthesis: clinical and radiographic results in six patients.Spine (Phila Pa 1976). 2002 Mar 15;27(6):E161-8. doi: 10.1097/00007632-200203150-00019. Spine (Phila Pa 1976). 2002. PMID: 11884921
-
Minimally Invasive Surgery for Managing Grade IV and V Spondylolisthesis.Asian J Neurosurg. 2023 Sep 22;18(3):437-443. doi: 10.1055/s-0043-1771317. eCollection 2023 Sep. Asian J Neurosurg. 2023. PMID: 38152513 Free PMC article. Review.
Cited by
-
Clinical and Radiological Outcomes after Reducing Adult Lytic High-Grade Spondylolisthesis Using a Hybrid Technique: Combination of Percutaneous Pedicle Screws with Midline Microscopic Transforaminal Decompression.Asian Spine J. 2023 Dec;17(6):1004-1012. doi: 10.31616/asj.2023.0098. Epub 2023 Nov 10. Asian Spine J. 2023. PMID: 37946335 Free PMC article.
-
[Progress in treatment of high-grade spondylolisthesis].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 Feb 15;38(2):226-233. doi: 10.7507/1002-1892.202309051. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 38385237 Free PMC article. Review. Chinese.
-
Does the L5 spinal nerve move? Anatomical evaluation with implications for postoperative L5 nerve palsy.Surg Radiol Anat. 2021 Jun;43(6):813-818. doi: 10.1007/s00276-020-02578-5. Epub 2020 Sep 24. Surg Radiol Anat. 2021. PMID: 32970169
-
Surgical treatment of spondylolisthesis using long arm screw: A literature review.Ann Med Surg (Lond). 2021 Dec 21;73:103200. doi: 10.1016/j.amsu.2021.103200. eCollection 2022 Jan. Ann Med Surg (Lond). 2021. PMID: 35079357 Free PMC article. Review.
-
Increased Risk of Adjacent Segment Spondylolisthesis or Instability Following L5-S1 Versus L4-S1 Fixation for L5-S1 High-Grade Dysplastic Spondylolisthesis in Children.Orthop Surg. 2025 Apr;17(4):1133-1142. doi: 10.1111/os.14367. Epub 2025 Jan 22. Orthop Surg. 2025. PMID: 39840663 Free PMC article.
References
-
- Ralston S, Weir M. Suspecting lumbar spondylolysis in adolescent low back pain. Clin Pediatr. 1998;37(5):287–293. - PubMed
-
- Molinari RW, Bridwell KH, Lenke LG, et al. Complications in the surgical treatment of pediatric high-grade, isthmic dysplastic spondylolisthesis. A comparison of three surgical approaches. Spine (Phila Pa 1976) 1999;24(16):1701–1711. - PubMed
-
- Harms J, Jeszensky D, Stoltze D, et al. True spondylolisthesis reduction and monosegmental fusion in spondylolisthesis. In: Bridwell KH, DeWald RL, editors. The Textbook of Spinal Surgery 2nd ed. Philadelphia, PA: Lippincott-Raven Publishers;; 1997. pp. 1337–1347.
-
- Dewald RL, Taddonio RF, Neuwirth MG. Severe lumbosacral spondylolisthesis in adolescents and children. J Bone Joint Surg Am. 1981;63(4):619–626. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials