

Pharmacological management of post-traumatic seizures in adults: current practice patterns in the UK and the Republic of Ireland
- PMID: 30276544
- PMCID: PMC6407744
- DOI: 10.1007/s00701-018-3683-9
Pharmacological management of post-traumatic seizures in adults: current practice patterns in the UK and the Republic of Ireland
Abstract
Background: Patient selection for seizure prophylaxis after traumatic brain injury (TBI) and duration of anti-epileptic drug treatment for patients with early post-traumatic seizures (PTS), remain plagued with uncertainty. In early 2017, a collaborative group of neurosurgeons, neurologists, neurointensive care and rehabilitation medicine physicians was formed in the UK with the aim of assessing variability in current practice and gauging the degree of uncertainty to inform the design of future studies. Here we present the results of a survey of clinicians managing patients with TBI in the UK and Ireland.
Materials and methods: An online survey was developed and piloted. Following approval by the Academic Committee of the Society of British Neurological Surgeons, it was distributed via appropriate electronic mailing lists.
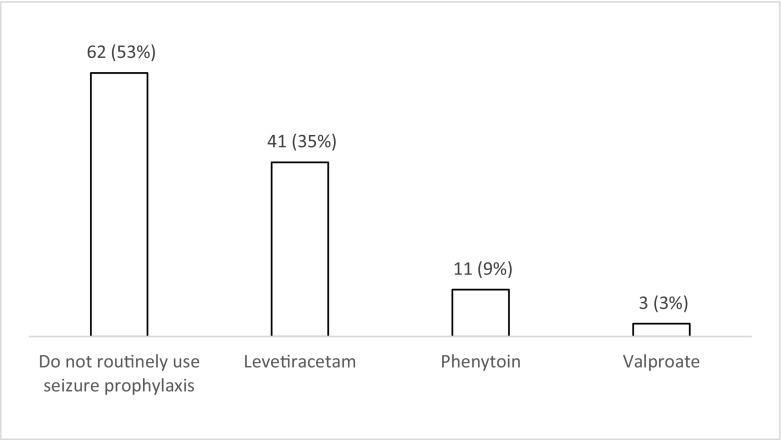
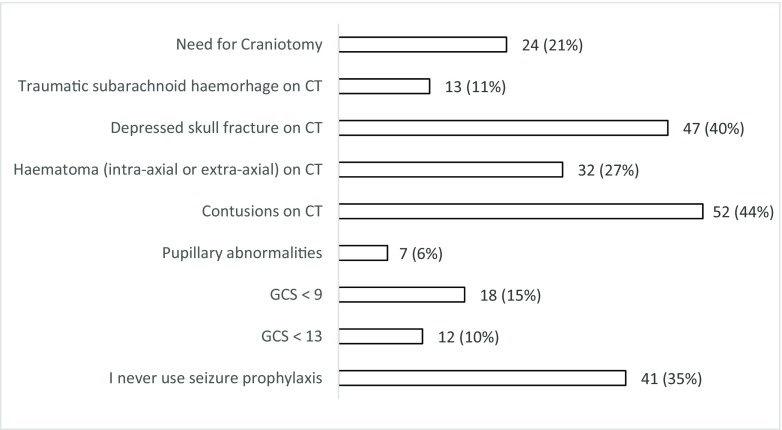
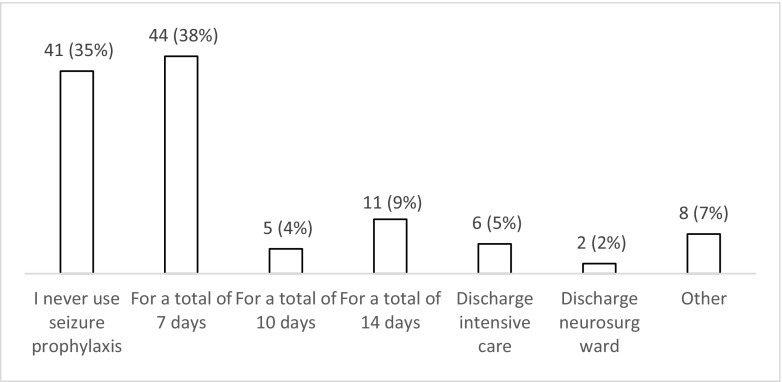
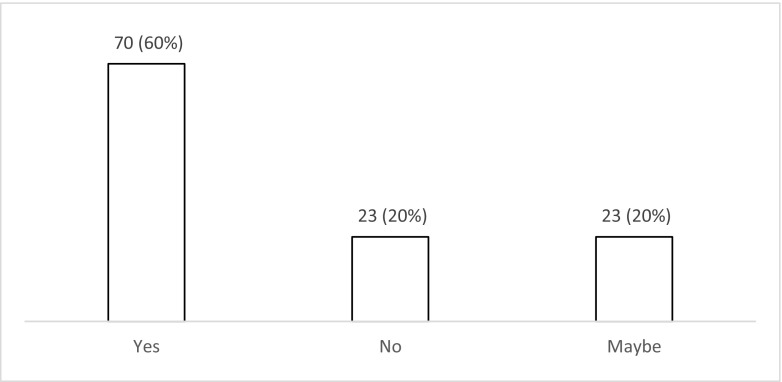
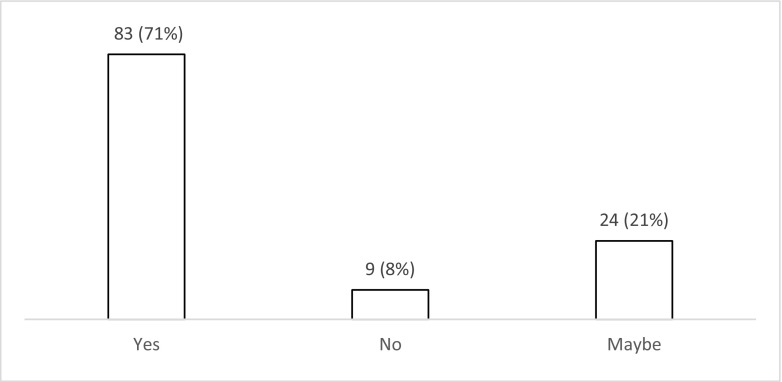
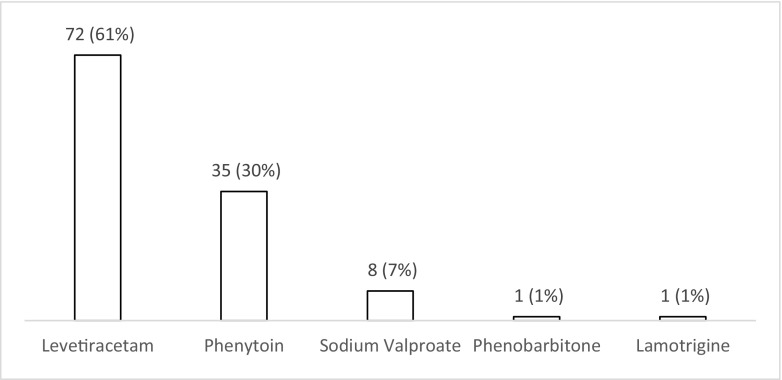
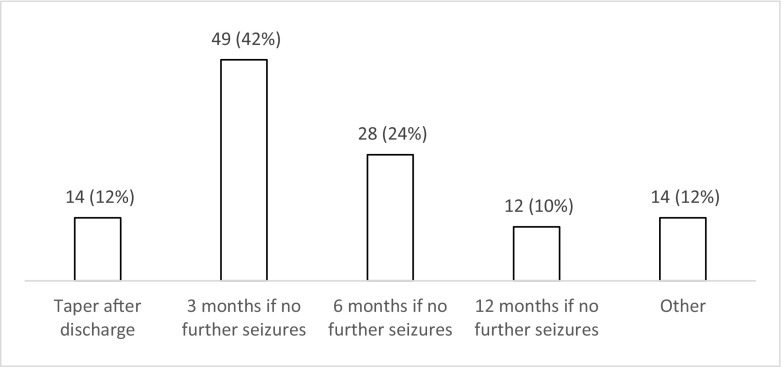
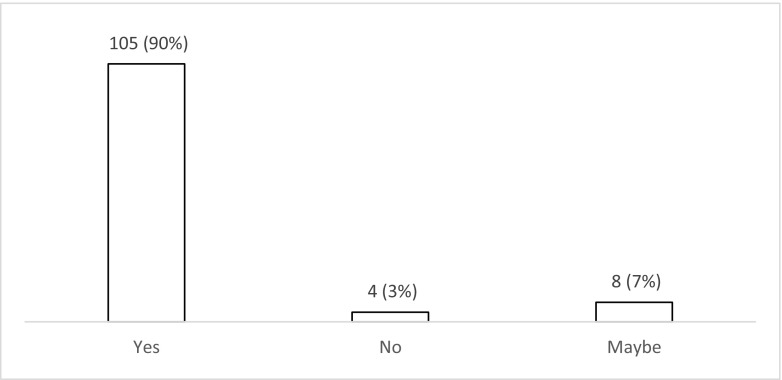
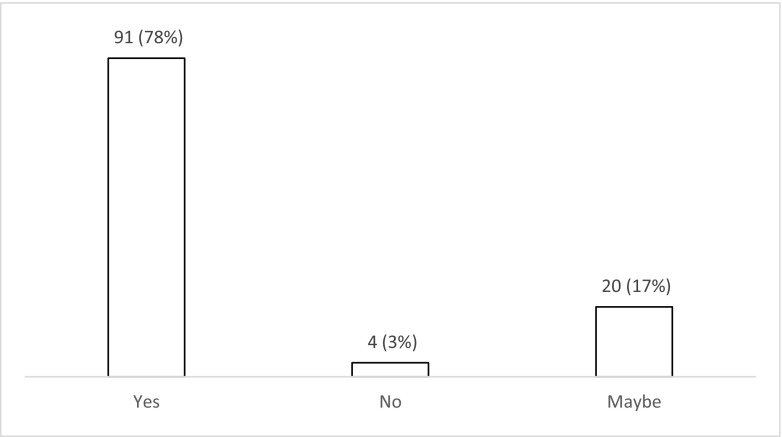
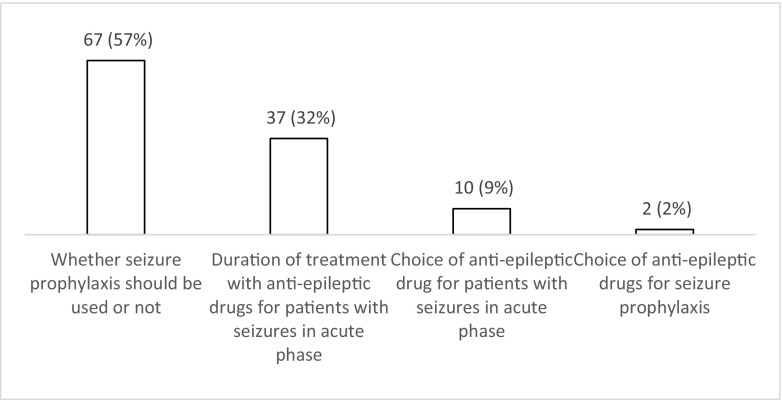
Results: One hundred and seventeen respondents answered the questionnaire, predominantly neurosurgeons (76%) from 30 (of 32) trauma-receiving hospitals in the UK and Ireland. Fifty-three percent of respondents do not routinely use seizure prophylaxis, but 38% prescribe prophylaxis for one week. Sixty percent feel there is uncertainty regarding the use of seizure prophylaxis, and 71% would participate in further research to address this question. Sixty-two percent of respondents use levetiracetam for treatment of seizures during the acute phase, and 42% continued for a total of 3 months. Overall, 90% were uncertain about the duration of treatment for seizures, and 78% would participate in further research to address this question.
Conclusion: The survey results demonstrate the variation in practice and uncertainty in both described aspects of management of patients who have suffered a TBI. The majority of respondents would want to participate in future research to help try and address this critical issue, and this shows the importance and relevance of these two clinical questions.
Keywords: Anti-epileptic medication; Post-traumatic seizures; Seizure prophylaxis; Traumatic brain injury.
Conflict of interest statement
Conflict of interest
All authors certify that they have no affiliations.
with or involvement in any organisation or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licencing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Figures
References
-
- Carney N, Totten A, OReilly C et al (2016) Guidelines for the management of severe traumatic brain injury. 1:1–244
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
