

Age-varying effects of cannabis use frequency and disorder on symptoms of psychosis, depression and anxiety in adolescents and adults
- PMID: 30276906
- PMCID: PMC6519223
- DOI: 10.1111/add.14459
Age-varying effects of cannabis use frequency and disorder on symptoms of psychosis, depression and anxiety in adolescents and adults
Abstract
Aims: We tested the age-varying associations of cannabis use (CU) frequency and disorder (CUD) with psychotic, depressive and anxiety symptoms in adolescent and adult samples. Moderating effects of early onset (≤ 15 years) and sex were tested.
Design: Time-varying effect models were used to assess the significance of concurrent associations between CU and CUD and symptoms of psychosis, depression and anxiety at each age.
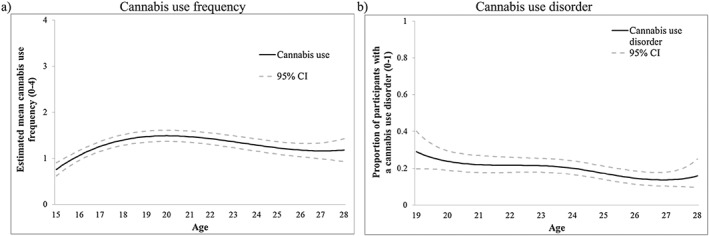
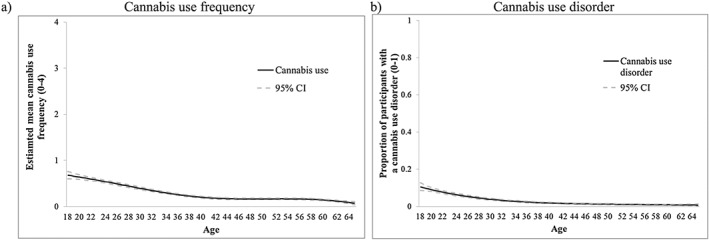
Setting and participants: Adolescent data (V-HYS; n = 662) were collected from a randomly recruited sample of adolescents in Victoria, British Columbia, Canada during a 10-year period (2003-13). Adult cross-sectional data (NESARC-III; n = 36 309) were collected from a representative sample from the United States (2012-13).
Measurements: Mental health symptoms were assessed using self-report measures of diagnostic symptoms. CU was based on frequency of past-year use. Past-year CUD was based on DSM-5 criteria.
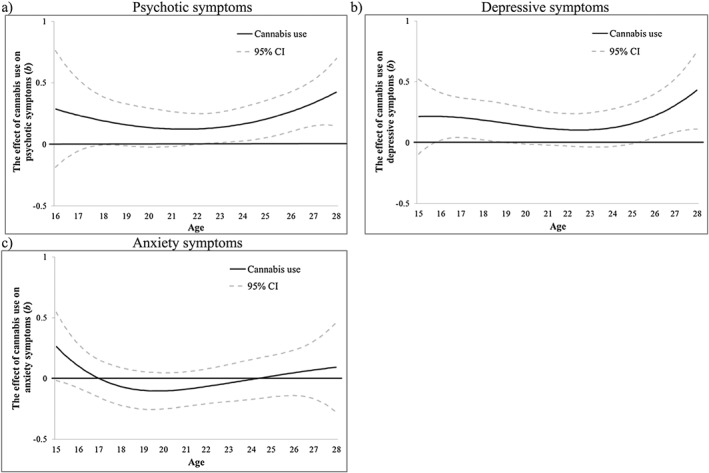
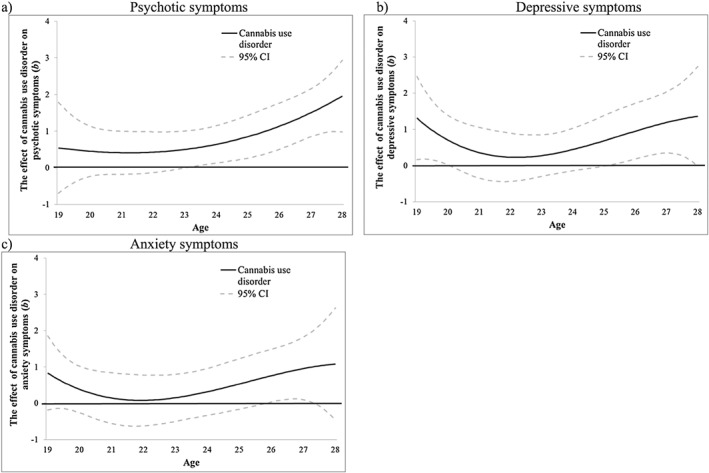
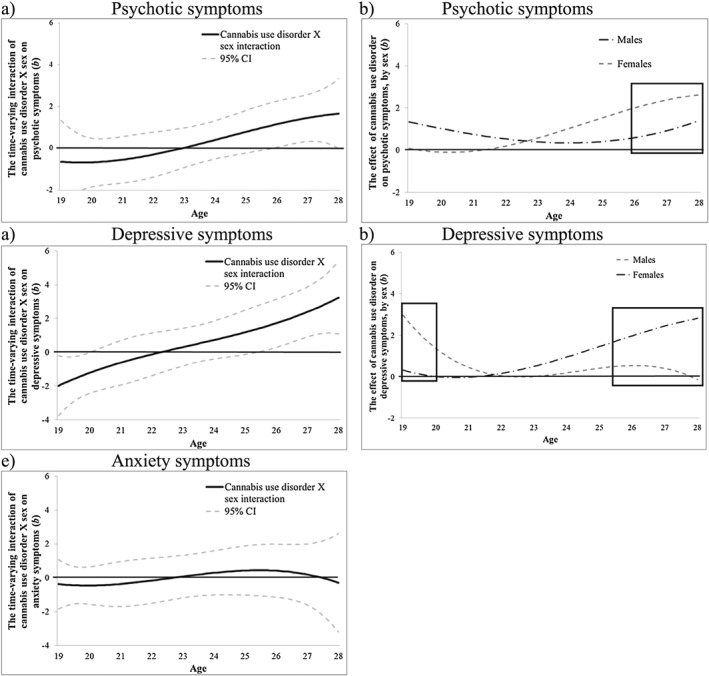
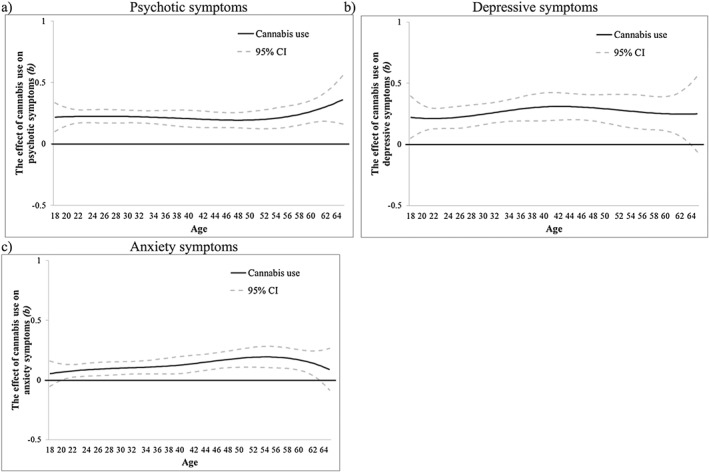
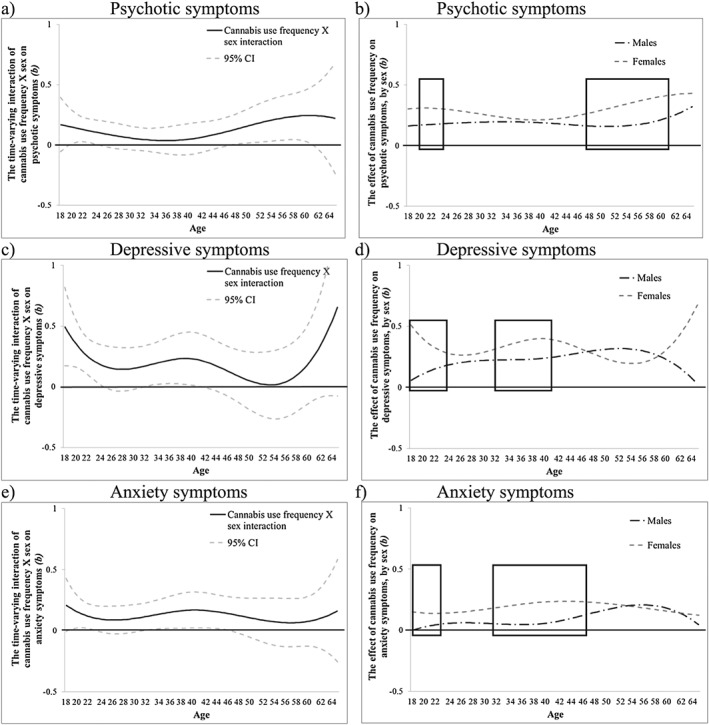
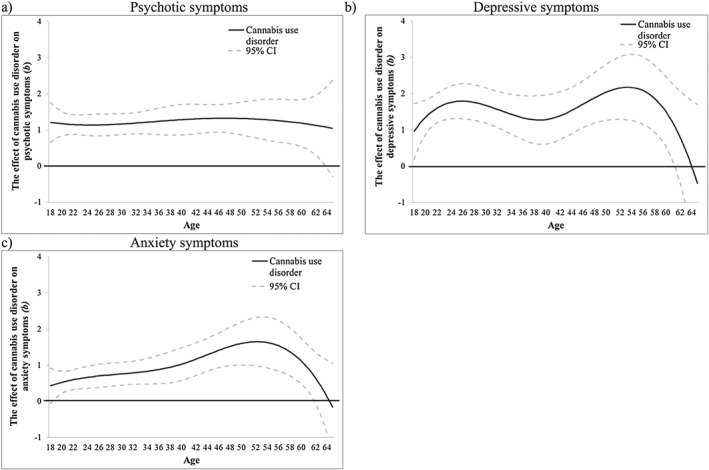
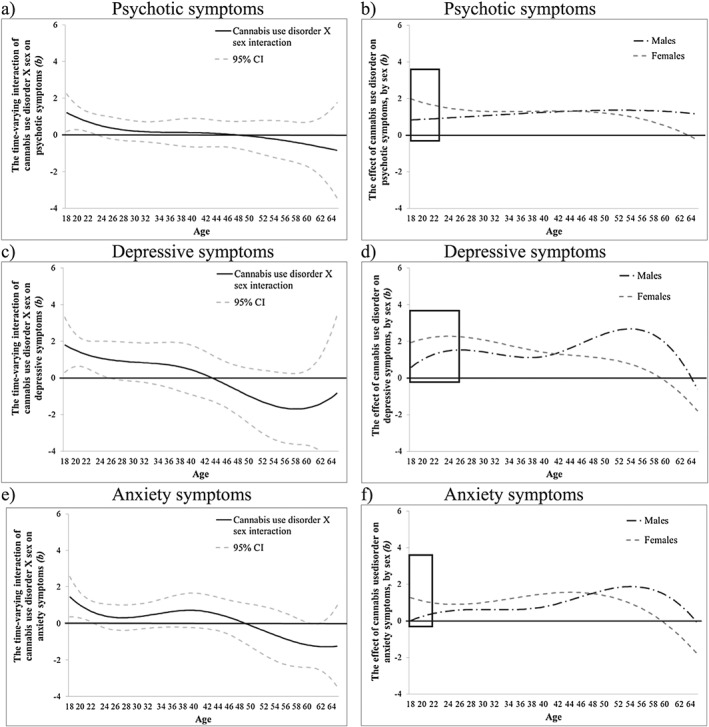
Findings: For youth in the V-HYS, CU was associated with psychotic symptoms following age 22 [b = 0.13, 95% confidence interval (CI) = 0.002, 0.25], with depressive symptoms from ages 16-19 and following age 25 (b = 0.17, 95% CI = 0.003, 0.34), but not with anxiety symptoms. CUD was associated with psychotic symptoms following age 23 (b = 0.51, 95% CI = 0.01, 1.01), depressive symptoms at ages 19-20 and following age 25 (b = 0.71, 95% CI = 0.001, 1.42) and anxiety symptoms ages 26-27 only. For adults in the NESARC-III, CU was associated with mental health symptoms at most ages [e.g. psychotic symptoms; age 18 (b = 0.22, 95% CI = 0.10, 0.33) to age 65 (b = 0.36, 95% CI = 0.16, 0.56)]. CUD was associated with all mental health symptoms across most ages [e.g. depressive symptoms; age 18 (b = 0.96, 95% CI = 0.19, 1.73) to age 61 (b = 1.11, 95% CI = 0.01, 2.21)]. Interactions with sex show stronger associations for females than males in young adulthood [e.g.
V-hys: CUD × sex interaction on psychotic symptoms significant after age 26 (b = 1.12, 95% CI = 0.02, 2.21)]. Findings were not moderated by early-onset CU.
Conclusions: Significant associations between cannabis use (CU) frequency and disorder (CUD) and psychotic and depressive symptoms in late adolescence and young adulthood extend across adulthood, and include anxiety.
Keywords: Adolescence; anxiety; cannabis use; cannabis use disorder; depression; early onset; marijuana; mental health; psychosis; young adulthood.
© 2018 The Authors. Addiction published by John Wiley & Sons Ltd on behalf of Society for the Study of Addiction.
Figures
References
-
- Gore F. M., Bloem P. J. N., Patton G. C., Ferguson J., Joseph V., Coffey C. et al Global burden of disease in young people aged 10–24 years: a systematic analysis. Lancet 2011; 377: 2093–2102. - PubMed
-
- Whiteford H. A., Degenhardt L., Rehm J., Baxter A. J., Ferrari A. J., Erskine H. E. et al Global burden of disease attributable to mental and substance use disorders: findings from the global burden of disease study 2010. Lancet 2013; 382: 1575–1586. - PubMed
-
- Hamilton I. Cannabis, psychosis and schizophrenia: unravelling a complex interaction. Addiction 2017; 112: 1653–1657. - PubMed
-
- Levine A., Clemenza K., Rynn M., Lieberman J. Evidence for the risks and consequences of adolescent cannabis exposure. J Am Acad Child Adolesc Psychiatry 2017; 56: 214–225. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
