

Randomized Feasibility Trial of a Low Tidal Volume-Airway Pressure Release Ventilation Protocol Compared With Traditional Airway Pressure Release Ventilation and Volume Control Ventilation Protocols
- PMID: 30277890
- PMCID: PMC6250244
- DOI: 10.1097/CCM.0000000000003437
Randomized Feasibility Trial of a Low Tidal Volume-Airway Pressure Release Ventilation Protocol Compared With Traditional Airway Pressure Release Ventilation and Volume Control Ventilation Protocols
Abstract
Objectives: Low tidal volume (= tidal volume ≤ 6 mL/kg, predicted body weight) ventilation using volume control benefits patients with acute respiratory distress syndrome. Airway pressure release ventilation is an alternative to low tidal volume-volume control ventilation, but the release breaths generated are variable and can exceed tidal volume breaths of low tidal volume-volume control. We evaluate the application of a low tidal volume-compatible airway pressure release ventilation protocol that manages release volumes on both clinical and feasibility endpoints.
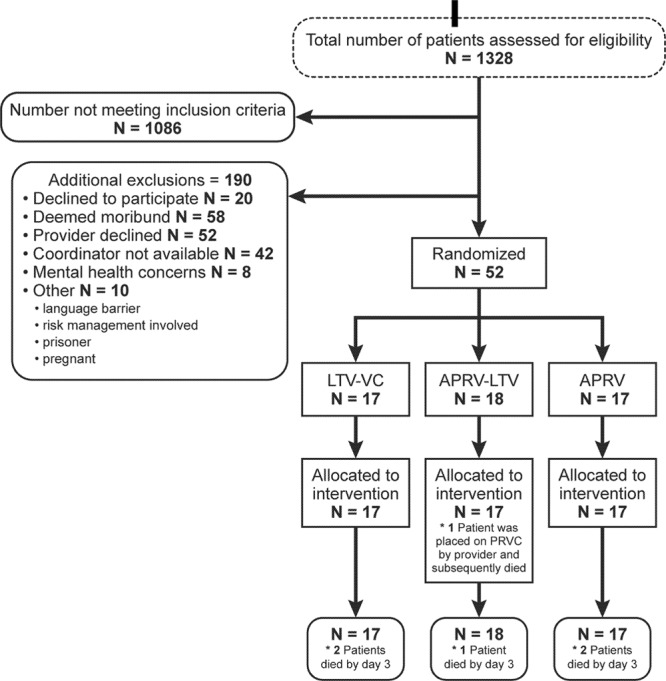
Design: We designed a prospective randomized trial in patients with acute hypoxemic respiratory failure. We randomized patients to low tidal volume-volume control, low tidal volume-airway pressure release ventilation, and traditional airway pressure release ventilation with a planned enrollment of 246 patients. The study was stopped early because of low enrollment and inability to consistently achieve tidal volumes less than 6.5 mL/kg in the low tidal volume-airway pressure release ventilation arm. Although the primary clinical study endpoint was PaO2/FIO2 on study day 3, we highlight the feasibility outcomes related to tidal volumes in both arms.
Setting: Four Intermountain Healthcare tertiary ICUs.
Patients: Adult ICU patients with hypoxemic respiratory failure anticipated to require prolonged mechanical ventilation.
Interventions: Low tidal volume-volume control, airway pressure release ventilation, and low tidal volume-airway pressure release ventilation.
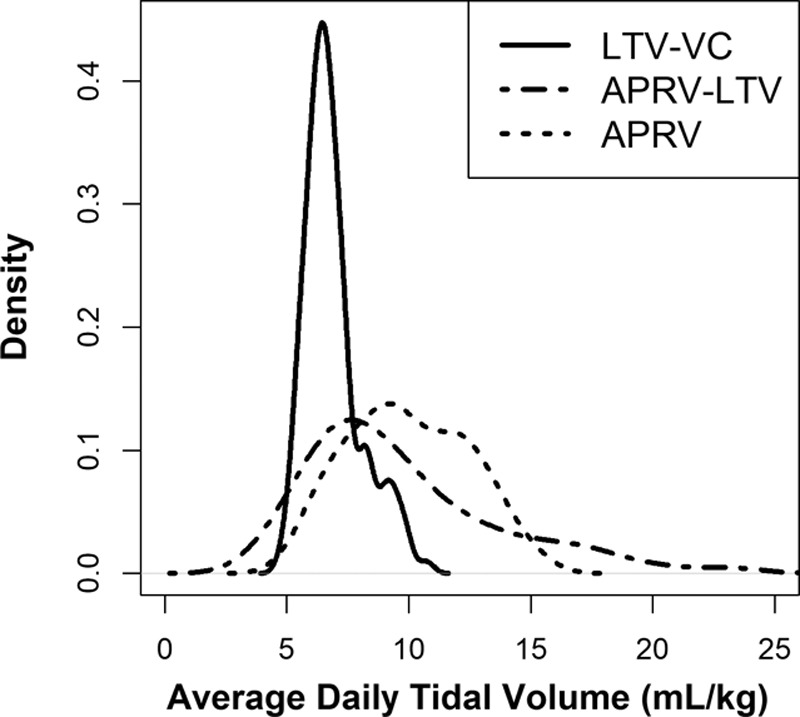
Measurements and main results: We observed wide variability and higher tidal (release for airway pressure release ventilation) volumes in both airway pressure release ventilation (8.6 mL/kg; 95% CI, 7.8-9.6) and low tidal volume-airway pressure release ventilation (8.0; 95% CI, 7.3-8.9) than volume control (6.8; 95% CI, 6.2-7.5; p = 0.005) with no difference between airway pressure release ventilation and low tidal volume-airway pressure release ventilation (p = 0.58). Recognizing the limitations of small sample size, we observed no difference in 52 patients in day 3 PaO2/ FIO2 (p = 0.92). We also observed no significant difference between arms in sedation, vasoactive medications, or occurrence of pneumothorax.
Conclusions: Airway pressure release ventilation resulted in release volumes often exceeding 12 mL/kg despite a protocol designed to target low tidal volume ventilation. Current airway pressure release ventilation protocols are unable to achieve consistent and reproducible delivery of low tidal volume ventilation goals. A large-scale efficacy trial of low tidal volume-airway pressure release ventilation is not feasible at this time in the absence of an explicit, generalizable, and reproducible low tidal volume-airway pressure release ventilation protocol.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
It Is Time to Treat the Patient and Not Just the Ventilator.Crit Care Med. 2019 Aug;47(8):e723-e724. doi: 10.1097/CCM.0000000000003782. Crit Care Med. 2019. PMID: 31305315 Free PMC article. No abstract available.
-
The authors reply.Crit Care Med. 2019 Aug;47(8):e724-e726. doi: 10.1097/CCM.0000000000003857. Crit Care Med. 2019. PMID: 31305316 No abstract available.
References
-
- Brower RG, Matthay MA, Morris A, et al. ; Acute Respiratory Distress Syndrome Network: Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000; 342:1301–1308. - PubMed
-
- Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med 1998; 338:347–354. - PubMed
-
- Gillette MA, Hess DR. Ventilator-induced lung injury and the evolution of lung-protective strategies in acute respiratory distress syndrome. Respir Care 2001; 46:130–148. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
