

Feasibility and Efficacy of Transient Elastography using the XL probe to diagnose liver fibrosis and cirrhosis: A meta-analysis
- PMID: 30278481
- PMCID: PMC6181481
- DOI: 10.1097/MD.0000000000011816
Feasibility and Efficacy of Transient Elastography using the XL probe to diagnose liver fibrosis and cirrhosis: A meta-analysis
Abstract
Background: Transient elastography (TE) has been validated as an effective noninvasive tool for the assessment of liver fibrosis. The XL probe is a new probe that was initially designed for use in patients with obesity. A meta-analysis was performed to assess the feasibility and efficacy of TE using the XL probe.
Methods: In September 2016, we systematically searched the PubMed and Science Direct search engines. The feasibility of TE was evaluated based on the failure rate and the results of the unreliable liver stiffness measurement (LSM). The efficacy of TE was measured using sensitivity, specificity, and summary receiver-operating characteristic as measures/indices assessed in different stages of fibrosis. Heterogeneity was measured using the chi-squared test and the Q-statistic. We used the 95% confidence interval (95% CI) as an effect measure.
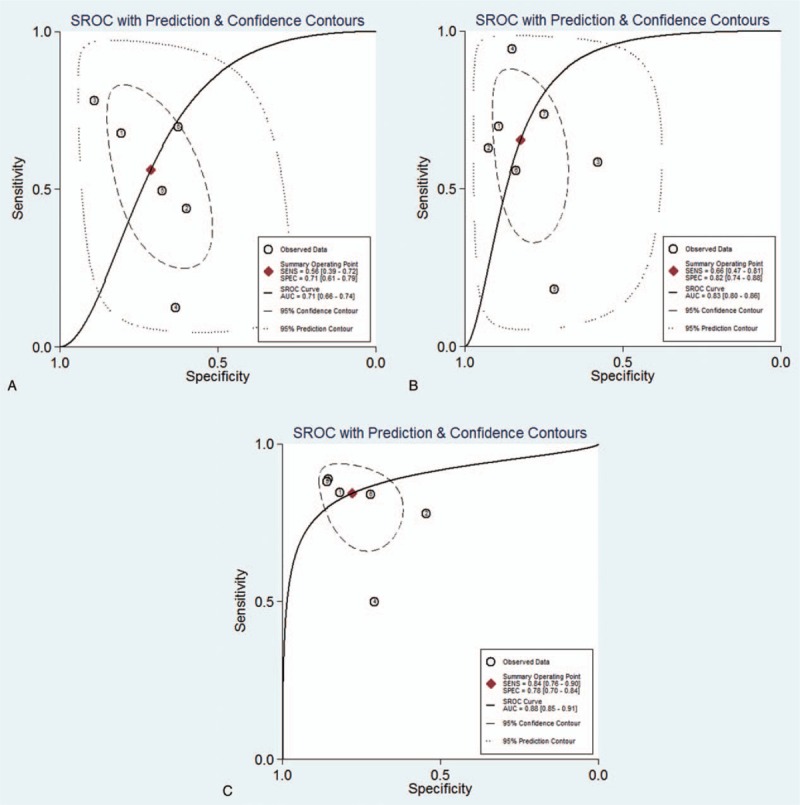
Results: We included 8 studies in the meta-analysis. When the XL was compared to the M probe, the former showed a lower risk of failure rate [relative risk (RR) 0.24, 95% CI 0.14-0.38]. In patients with a body mass index ≥30 kg/m, the XL probe showed a statistically significantly lower risk of failure rate (RR 0.16, 95% CI 0.08-0.32) but no significant improvement (RR 0.76, 95% CI 0.50-1.16) in the unreliable LSM result. In patients showing liver fibrosis stage ≥F2, the XL probe showed a sensitivity of 0.56 (95% CI 0.39-0.72), specificity of 0.71 (95% CI 0.61-0.79), and an area under the curve (AUC) of 0.71. The results observed in patients with liver fibrosis stage F4 were more promising with a sensitivity of 0.84 (95% CI 0.76-0.90), specificity of 0.78 (95% CI 0.70-0.84), and an AUC of 0.88.
Conclusion: TE using the XL probe demonstrates significant diagnostic utility in patients with liver fibrosis and is likely to be more reliable than the M probe in patients with obesity. Large prospective multicenter studies are, however, necessary to establish the new cut-off values to be used for the XL probe in patients with obesity.
Conflict of interest statement
The authors report no conflicts of interest.
Figures


References
-
- Nguyen-Khac E. Results and place of Fibroscan in the non-invasive diagnosis of hepatic fibrosis. Rev Med Interne 2007;28:94–102. - PubMed
-
- De Franchis R, Dell’Era A. Non-invasive diagnosis of cirrhosis and the natural history of its complications. Best Pract Res Clin Gastroenterol 2007;21:3–18. - PubMed
-
- Cadranel JF, Rufat P, Degos F. Practices of liver biopsy in France: results of a prospective nationwide survey. For the Group of Epidemiology of the French Association for the Study of the Liver (AFEF). Hepatology 2000;32:477–81. - PubMed
-
- Bedossa P, Dargere D, Paradis V. Sampling variability of liver fibrosis in chronic hepatitis C. Hepatology 2003;38:1449–57. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
