

Age-Related Changes in HAPLN1 Increase Lymphatic Permeability and Affect Routes of Melanoma Metastasis
- PMID: 30279172
- PMCID: PMC6328344
- DOI: 10.1158/2159-8290.CD-18-0168
Age-Related Changes in HAPLN1 Increase Lymphatic Permeability and Affect Routes of Melanoma Metastasis
Abstract
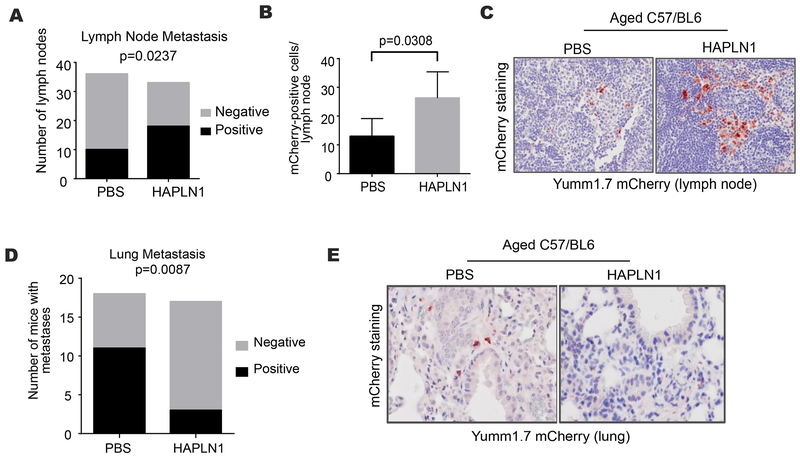
Older patients with melanoma have lower rates of sentinel lymph node (LN) metastases yet paradoxically have inferior survival. Patient age correlated with an inability to retain Technetium radiotracer during sentinel LN biopsy in more than 1,000 patients, and high Technetium counts correlated to better survival. We hypothesized that loss of integrity in the lymphatic vasculature due to extracellular matrix (ECM) degradation might play a role. We have implicated HAPLN1 in age-dependent ECM degradation in the dermis. Here, we queried whether HAPLN1 could be altered in the lymphatic ECM. Lymphatic HAPLN1 expression was prognostic of long-term patient survival. Adding recombinant HAPLN1 to aged fibroblast ECMs in vitro reduced endothelial permeability via modulation of VE-cadherin junctions, whereas endothelial permeability was increased following HAPLN1 knockdown in young fibroblasts. In vivo, reconstitution of HAPLN1 in aged mice increased the number of LN metastases, but reduced visceral metastases. These data suggest that age-related changes in ECM can contribute to impaired lymphatics. SIGNIFICANCE: Our studies reveal that changes in the stroma during aging may influence the way tumor cells traffic through the lymphatic vasculature. Aging may dictate the route of metastatic dissemination of tumor cells, and understanding these changes may help to reveal targetable moieties in the aging tumor microenvironment.See related commentary by Marie and Merlino, p. 19.This article is highlighted in the In This Issue feature, p. 1.
©2018 American Association for Cancer Research.
Conflict of interest statement
Figures





Comment in
-
Something Old, Something New: The Tumor Microenvironment Comes of Age.Cancer Discov. 2019 Jan;9(1):19-21. doi: 10.1158/2159-8290.CD-18-1320. Cancer Discov. 2019. PMID: 30626604 Free PMC article.
References
-
- Balch CM, Soong SJ, Gershenwald JE, Thompson JF, Reintgen DS, Cascinelli N, et al. Prognostic factors analysis of 17,600 melanoma patients: validation of the American Joint Committee on Cancer melanoma staging system. J Clin Oncol. 2001;19:3622–34. - PubMed
-
- Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67:93–9. - PubMed
-
- Lasithiotakis K, Leiter U, Meier F, Eigentler T, Metzler G, Moehrle M, et al. Age and gender are significant independent predictors of survival in primary cutaneous melanoma. Cancer. 2008;112:1795–804. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
