

Long-read sequencing identified a causal structural variant in an exome-negative case and enabled preimplantation genetic diagnosis
- PMID: 30279644
- PMCID: PMC6162922
- DOI: 10.1186/s41065-018-0069-1
Long-read sequencing identified a causal structural variant in an exome-negative case and enabled preimplantation genetic diagnosis
Abstract
Background: For a proportion of individuals judged clinically to have a recessive Mendelian disease, only one heterozygous pathogenic variant can be found from clinical whole exome sequencing (WES), posing a challenge to genetic diagnosis and genetic counseling. One possible reason is the limited ability to detect disease causal structural variants (SVs) from short reads sequencing technologies. Long reads sequencing can produce longer reads (typically 1000 bp or longer), therefore offering greatly improved ability to detect SVs that may be missed by short-read sequencing.
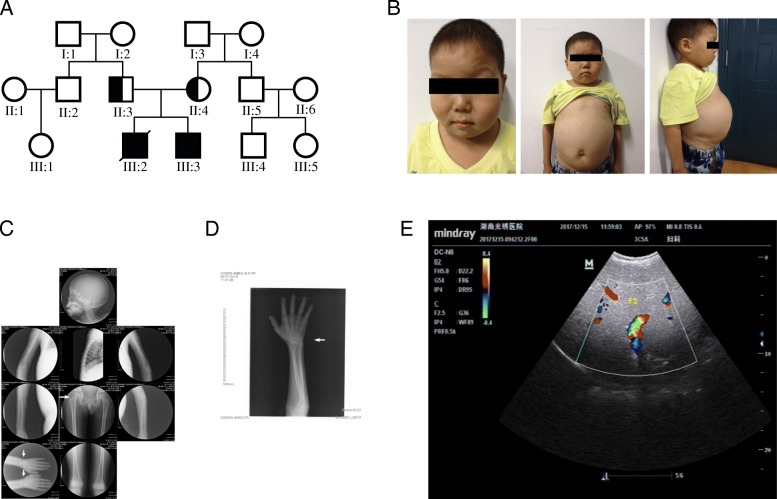
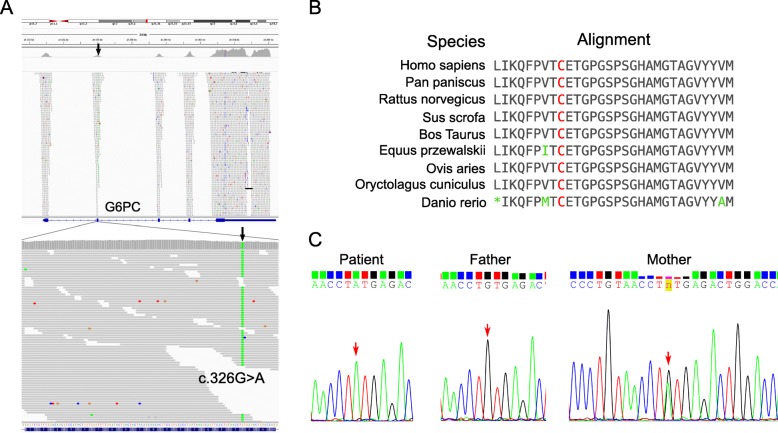
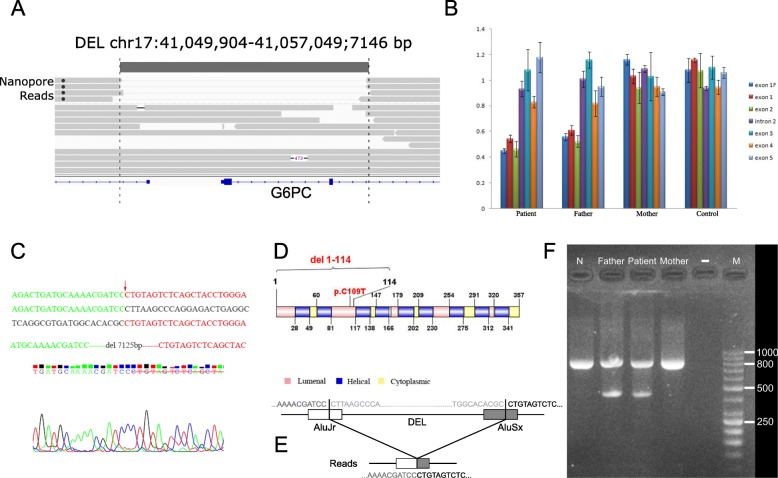
Results: Here we describe a case study, where WES identified only one heterozygous pathogenic variant for an individual suspected to have glycogen storage disease type Ia (GSD-Ia), which is an autosomal recessive disease caused by bi-allelic mutations in the G6PC gene. Through Nanopore long-read whole-genome sequencing, we identified a 7.1 kb deletion covering two exons on the other allele, suggesting that complex structural variants (SVs) may explain a fraction of cases when the second pathogenic allele is missing from WES on recessive diseases. Both breakpoints of the deletion are within Alu elements, and we designed Sanger sequencing and quantitative PCR assays based on the breakpoints for preimplantation genetic diagnosis (PGD) for the family planning on another child. Four embryos were obtained after in vitro fertilization (IVF), and an embryo without deletion in G6PC was transplanted after PGD and was confirmed by prenatal diagnosis, postnatal diagnosis, and subsequent lack of disease symptoms after birth.
Conclusions: In summary, we present one of the first examples of using long-read sequencing to identify causal yet complex SVs in exome-negative patients, which subsequently enabled successful personalized PGD.
Keywords: G6PC; GSD-Ia; Long-read sequencing; PGD; Structural variants; WES; Whole-exome sequencing.
Conflict of interest statement
The research including human subjects, human material, human data, has been performed in accordance with the Declaration of Helsinki and was approved by the ethics committee of Reproductive and Genetic Hospital of CITIC-Xiangya.The research contains individual person’s data (including detailed clinical phenotypes and images) and we have obtained consent from parents of the children.J.Z., Q.Y., F.L., D.W. are employees and K.W. is consultant of Grandomics Biosciences. All the other authors have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Trujillano D, Bertoli-Avella AM, Kumar Kandaswamy K, Weiss ME, Koster J, Marais A, Paknia O, Schroder R, Garcia-Aznar JM, Werber M, et al. Clinical exome sequencing: results from 2819 samples reflecting 1000 families. Eur J Hum Genet. 2017;25(2):176–182. doi: 10.1038/ejhg.2016.146. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
