

The Use of a Free Fibular Strut as a "Biological Intramedullary Nail" for the Treatment of Complex Nonunion of Long Bones
- PMID: 30280135
- PMCID: PMC6145563
- DOI: 10.2106/JBJS.OA.17.00050
The Use of a Free Fibular Strut as a "Biological Intramedullary Nail" for the Treatment of Complex Nonunion of Long Bones
Abstract
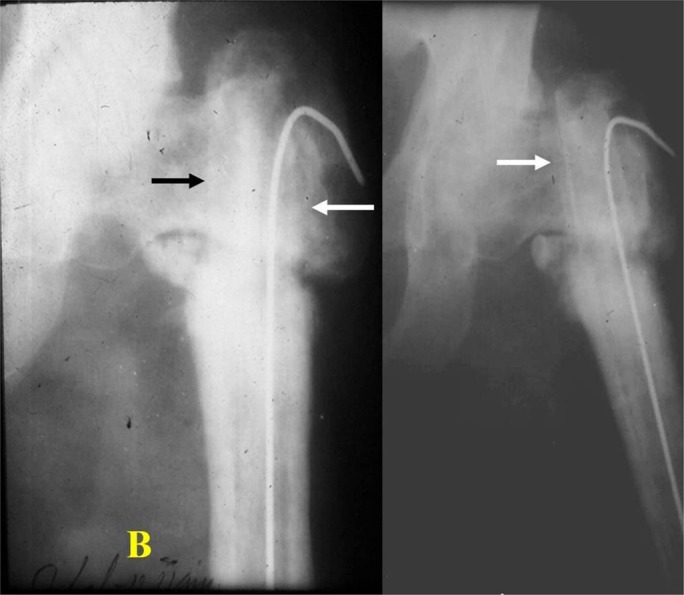
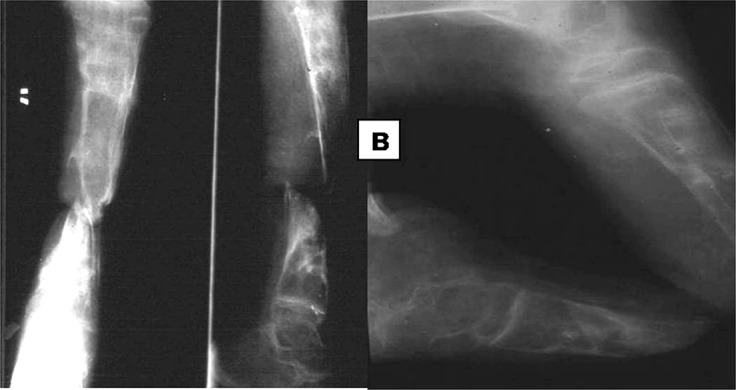
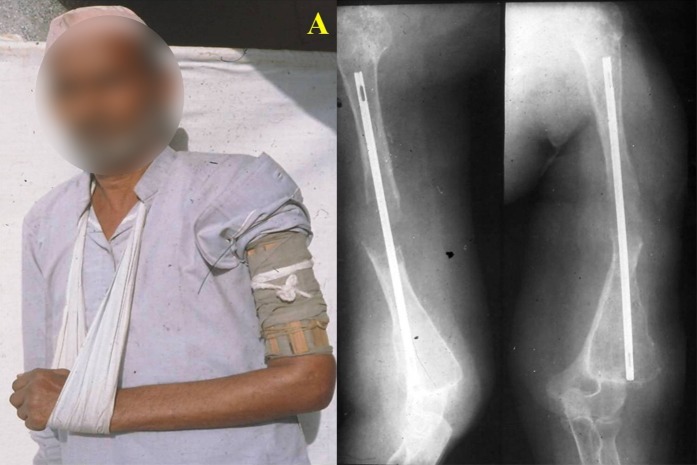
Background: Nonunion of long-bone fractures is difficult to treat, especially when the bones are osteoporotic or there is a large bone gap as a result of repeated failure of the metallic nails or implants. In such cases, the use of an autologous intramedullary fibular strut graft may be a viable treatment option.
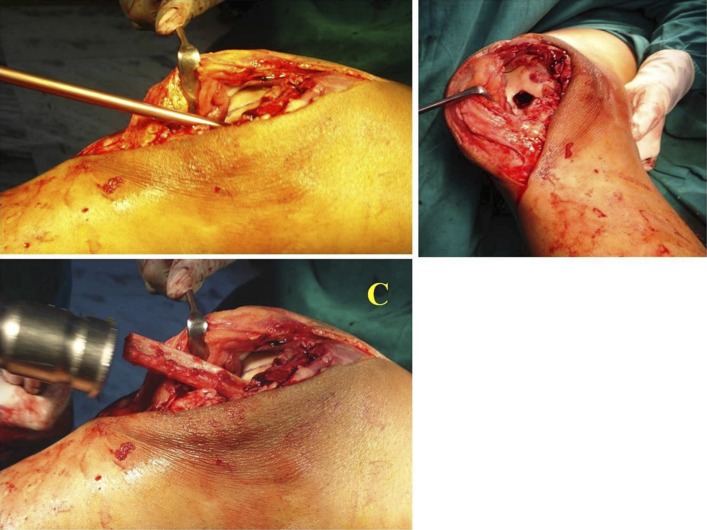
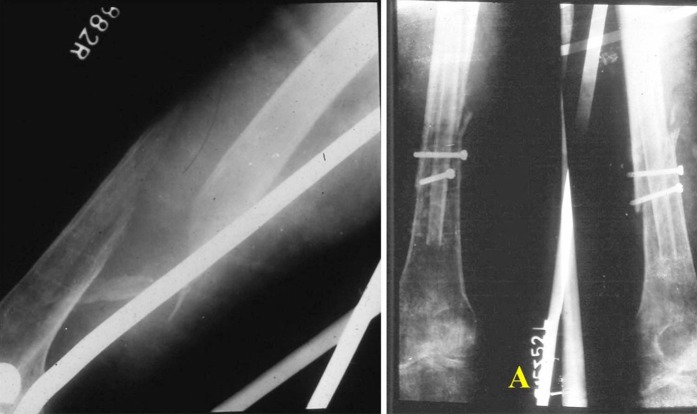
Methods: Twenty-two patients with a complex nonunion of the shaft of the femur, humerus, or tibia were managed with a free autologous fibular strut graft for intramedullary fixation with use of closed or open methods. All patients had evidence of moderate to severe local osteoporosis and had a bone gap ranging from 4 to 20 mm. Nineteen patients had had 1 to 4 prior operations. The mean age was 51.5 years. The duration of nonunion ranged from 9 months to 4 years.
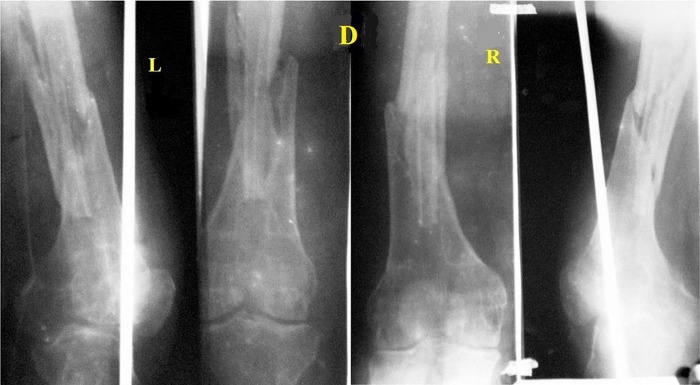
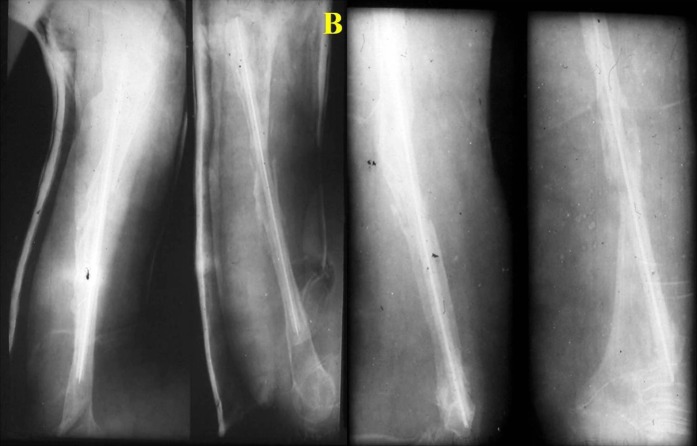
Results: The mean time to union was 17 weeks (range, 8 to 26 weeks), and the mean duration of follow-up was 4 years (range, 6 months to 17 years). All but 2 patients had healing at the time of the latest follow-up.
Conclusions: The identification of a viable option for the treatment of difficult nonunion in osteoporotic bones has been a challenge. The insertion of a free autologous intramedullary fibular strut graft provided mechanical stability, and osteogenesis occurred inside the medullary canal of the host bone.
Level of evidence: Therapeutic Level IV. See Instructions for Authors for a complete description of levels of evidence.
Figures








Similar articles
-
Role of autologous non-vascularised intramedullary fibular strut graft in humeral shaft nonunions following failed plating.J Clin Orthop Trauma. 2017 Nov;8(Suppl 2):S21-S30. doi: 10.1016/j.jcot.2016.12.006. Epub 2016 Dec 22. J Clin Orthop Trauma. 2017. PMID: 29339841 Free PMC article.
-
Gap nonunion of forearm bones treated by modified Nicoll's technique.Indian J Orthop. 2010 Jan;44(1):84-8. doi: 10.4103/0019-5413.58611. Indian J Orthop. 2010. PMID: 20165682 Free PMC article.
-
Randomized, prospective comparison of plate versus intramedullary nail fixation for distal tibia shaft fractures.J Orthop Trauma. 2011 Dec;25(12):736-41. doi: 10.1097/BOT.0b013e318213f709. J Orthop Trauma. 2011. PMID: 21904230 Clinical Trial.
-
Does Screw Configuration or Fibular Osteotomy Decrease Healing Time in Exchange Tibial Nailing?J Orthop Trauma. 2016 Nov;30(11):622-626. doi: 10.1097/BOT.0000000000000647. J Orthop Trauma. 2016. PMID: 27437613 Review.
-
The use of gentamicin-coated nails in complex open tibia fracture and revision cases: A retrospective analysis of a single centre case series and review of the literature.Injury. 2015 Dec;46(12):2433-7. doi: 10.1016/j.injury.2015.09.028. Epub 2015 Oct 8. Injury. 2015. PMID: 26477343 Review.
Cited by
-
The Pedicled Fibula Flap for Lower Limb Reconstruction.Strategies Trauma Limb Reconstr. 2023 Sep-Dec;18(3):186-193. doi: 10.5005/jp-journals-10080-1600. Strategies Trauma Limb Reconstr. 2023. PMID: 38404565 Free PMC article.
-
Giant cell tumor of proximal femur managed by extended curettage with fibular strut allograft using long intramedullary interlocking nail: A case report and literature review.Medicine (Baltimore). 2024 Dec 13;103(50):e40960. doi: 10.1097/MD.0000000000040960. Medicine (Baltimore). 2024. PMID: 39686440 Free PMC article. Review.
-
Fibular strut graft placement for an open distal femur fracture with a critical bone defect: A case report.Trauma Case Rep. 2022 Oct 4;42:100712. doi: 10.1016/j.tcr.2022.100712. eCollection 2022 Dec. Trauma Case Rep. 2022. PMID: 36210920 Free PMC article.
-
Resistant and Refractory Distal Tibia Non-Union Using an Intramedullary Free Fibular Graft and Ilizarov Fixation - An Illustrative Case Report.J Orthop Case Rep. 2024 Nov;14(11):45-49. doi: 10.13107/jocr.2024.v14.i11.4910. J Orthop Case Rep. 2024. PMID: 39524282 Free PMC article.
-
Autologous non-vascularized fibula with compression plating in the management of aseptic complex non-union of long bones.Int J Burns Trauma. 2024 Aug 25;14(4):75-83. doi: 10.62347/DQLS6083. eCollection 2024. Int J Burns Trauma. 2024. PMID: 39310247 Free PMC article.
References
-
- Trotter DH, Dobozi W. Nonunion of the humerus: rigid fixation, bone grafting, and adjunctive bone cement. Clin Orthop Relat Res. 1986. March;(204):162-8. - PubMed
-
- Rosen H. The treatment of nonunions and pseudarthroses of the humeral shaft. Orthop Clin North Am. 1990. October;21(4):725-42. - PubMed
-
- Wright TW, Miller GJ, Vander Griend RA, Wheeler D, Dell PC. Reconstruction of the humerus with an intramedullary fibular graft. A clinical and biomechanical study. J Bone Joint Surg Br. 1993. September;75(5):804-7. - PubMed
-
- Lynch JR, Taitsman LA, Barei DP, Nork SE. Femoral nonunion: risk factors and treatment options. J Am Acad Orthop Surg. 2008. February;16(2):88-97. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous