

Different Secretory Activity of Articular and Subcutaneous Adipose Tissues from Rheumatoid Arthritis and Osteoarthritis Patients
- PMID: 30280295
- PMCID: PMC6394603
- DOI: 10.1007/s10753-018-0901-9
Different Secretory Activity of Articular and Subcutaneous Adipose Tissues from Rheumatoid Arthritis and Osteoarthritis Patients
Abstract
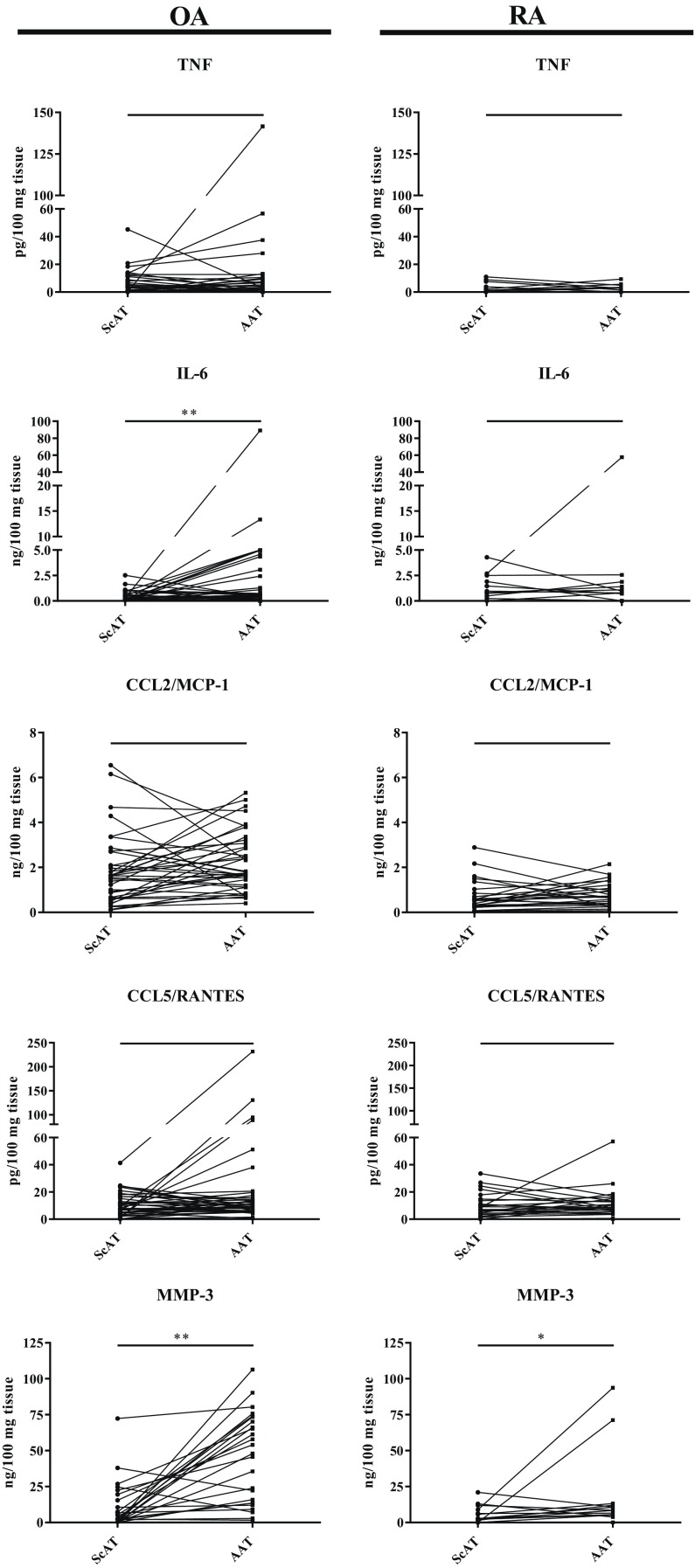
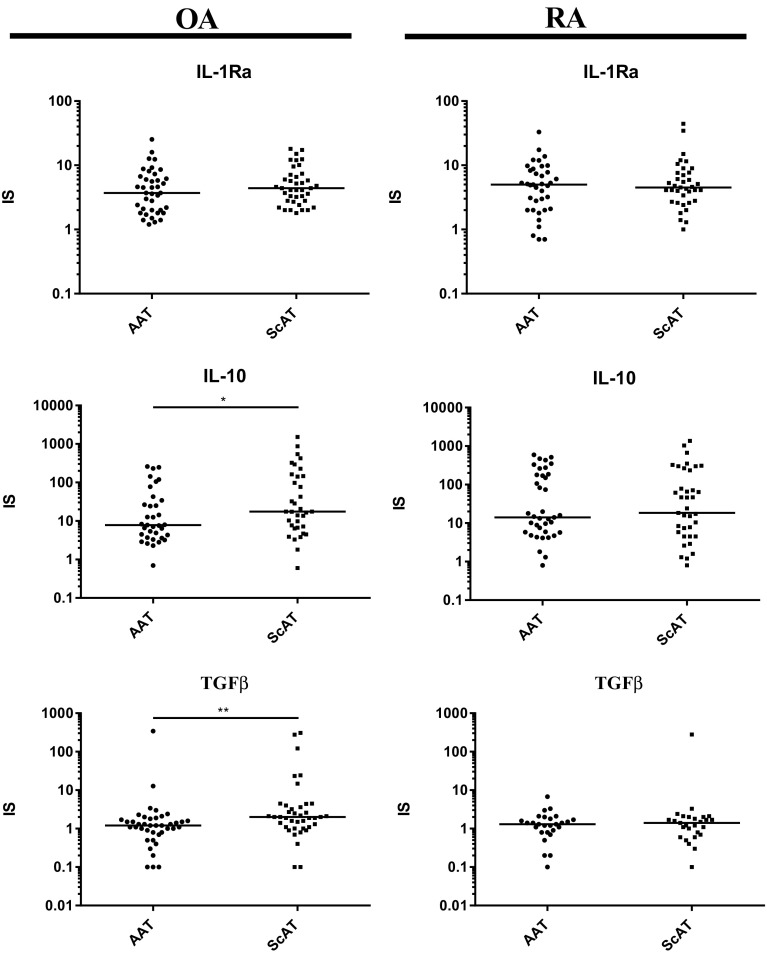
Rheumatoid arthritis (RA) and osteoarthritis (OA) are characterized by joint and systemic high- or low-grade inflammation, respectively. Adipose tissue (AT) may contribute to the pathogenesis of these diseases. To address this issue, we investigated whether basal and pro-inflammatory cytokine (IL-1β)-triggered release of adipocytokines (TNF, IL-6, IL-10, IL-1Ra, TGFβ, CCL2/MCP-1, CCL5/RANTES, MMP-3) from subcutaneous (ScAT) and intraarticular (AAT) adipose tissues of RA and OA patients mirror differences between these diseases in an intensity of systemic and local inflammation. We found that in both diseases basal adipocytokine release was usually higher from AAT than ScAT, reflecting stronger local than systemic inflammation. However, ScAT secreted considerable amounts of pro- and anti-inflammatory factors as well. Spontaneous secretion of some adipocytokines (MMP-3 and/or TNF, CCL2/MCP-1, IL-1Ra) was higher in osteoarthritis than rheumatoid ATs and probably caused by weaker anti-inflammatory treatment of OA patients. By contrast, reactivity of ATs to IL-1β was significantly lower in OA than RA and IL-1β antagonist (IL-1Ra) could be responsible for this because we found its overproduction in OA ATs. Interestingly, higher reactivity of ScAT than AAT to IL-1β was a characteristic for OA while reactivity of rheumatoid ScAT and AAT to this stimulus was equal. We conclude that differences between OA and RA in reactivity of AAT and ScAT to pro-inflammatory stimulus mimicking in vivo condition reflect dissimilarity in an intensity of disease-specific inflammation and thus support contribution of ATs to these pathological processes. Moreover, we propose that more efficient anti-inflammatory mechanism(s) are preserved in ATs of OA than RA patients.
Keywords: articular adipose tissue; chemokines; cytokines; osteoarthritis; rheumatoid arthritis; subcutaneous adipose tissue.
Figures


Similar articles
-
Articular adipose tissue resident macrophages in rheumatoid arthritis patients: potential contribution to local abnormalities.Rheumatology (Oxford). 2013 Dec;52(12):2158-67. doi: 10.1093/rheumatology/ket287. Epub 2013 Sep 6. Rheumatology (Oxford). 2013. PMID: 24014647
-
Comparison of rheumatoid articular adipose and synovial tissue reactivity to proinflammatory stimuli: contribution to adipocytokine network.Ann Rheum Dis. 2012 Feb;71(2):262-7. doi: 10.1136/annrheumdis-2011-200123. Epub 2011 Oct 11. Ann Rheum Dis. 2012. PMID: 21989538
-
Distinct Secretory Activity and Clinical Impact of Subcutaneous Abdominal Adipose Tissue in Women with Rheumatoid Arthritis and Osteoarthritis.Inflammation. 2017 Feb;40(1):106-116. doi: 10.1007/s10753-016-0459-3. Inflammation. 2017. PMID: 27796618
-
The role of cytokines in osteoarthritis pathophysiology.Biorheology. 2002;39(1-2):237-46. Biorheology. 2002. PMID: 12082286 Review.
-
Pro-inflammatory cytokines: The link between obesity and osteoarthritis.Cytokine Growth Factor Rev. 2018 Dec;44:38-50. doi: 10.1016/j.cytogfr.2018.10.002. Epub 2018 Oct 11. Cytokine Growth Factor Rev. 2018. PMID: 30340925 Review.
Cited by
-
Synovial fluid o-tyrosine is a potential biomarker for autoimmune-driven rheumatoid arthritis.Clin Rheumatol. 2025 Jul;44(7):2657-2668. doi: 10.1007/s10067-025-07491-z. Epub 2025 May 31. Clin Rheumatol. 2025. PMID: 40450162 Free PMC article.
-
Adipose-Derived Mesenchymal Stem Cells from Arthritis Patients: Differential Modulation of CD4⁺ T Cell Activation and Cytokine Production.Med Sci Monit. 2024 Nov 15;30:e945273. doi: 10.12659/MSM.945273. Med Sci Monit. 2024. PMID: 39543859 Free PMC article.
-
The burden of metabolic syndrome on osteoarthritic joints.Arthritis Res Ther. 2019 Dec 16;21(1):289. doi: 10.1186/s13075-019-2081-x. Arthritis Res Ther. 2019. PMID: 31842972 Free PMC article. Review.
-
A Metalloproteinase Induces an Inflammatory Response in Preadipocytes with the Activation of COX Signalling Pathways and Participation of Endogenous Phospholipases A2.Biomolecules. 2021 Jun 22;11(7):921. doi: 10.3390/biom11070921. Biomolecules. 2021. PMID: 34206390 Free PMC article.
-
Thigh muscle composition changes in knee osteoarthritis patients during weight loss: Sex-specific analysis using data from osteoarthritis initiative.Osteoarthritis Cartilage. 2024 Sep;32(9):1154-1162. doi: 10.1016/j.joca.2024.05.013. Epub 2024 Jun 6. Osteoarthritis Cartilage. 2024. PMID: 38851527 Free PMC article.
References
-
- Bui, Viet L., and Ernie Brahn. 2018. Cytokine targeting in rheumatoid arthritis. Clinical Immunology. 10.1016/j.clim.2018.04.001. - PubMed
-
- Rouhin Sen, and John A. Hurley. 2018. Osteoarthritis. StatPearls Publishing. - PubMed
-
- Angelotti F, Parma A, Cafaro G, Capecchi R, Alunno A, Puxeddu I. One year in review 2017: pathogenesis of rheumatoid arthritis. Clinical and Experimental Rheumatology. 2017;35:368–378. - PubMed
-
- Gisela B, Günther KP, Brenner H, Puhl W, Stürmer T, Rothenbacher D, Brenner RE. Osteoarthritis-patterns, cardio-metabolic risk factors and risk of all-cause mortality: 20 years follow-up in patients after hip or knee replacement. Scientific Reports. 2018;8:5253. doi: 10.1038/s41598-018-23573-2. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
