

Skeletal muscle fibrosis is associated with decreased muscle inflammation and weakness in patients with chronic kidney disease
- PMID: 30280599
- PMCID: PMC6336993
- DOI: 10.1152/ajprenal.00314.2018
Skeletal muscle fibrosis is associated with decreased muscle inflammation and weakness in patients with chronic kidney disease
Abstract
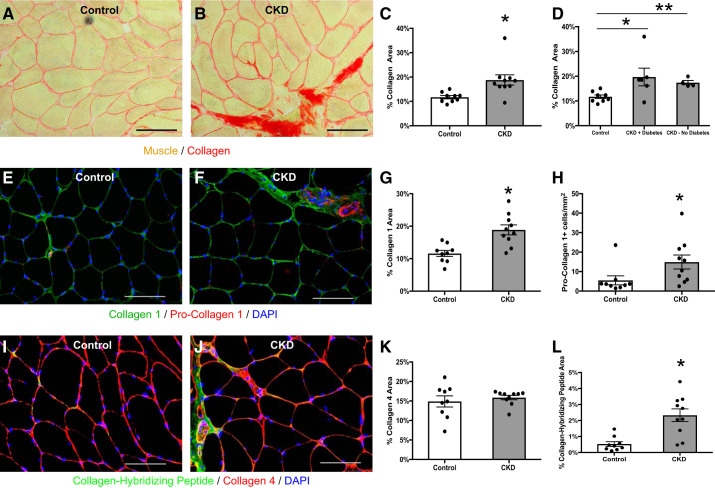
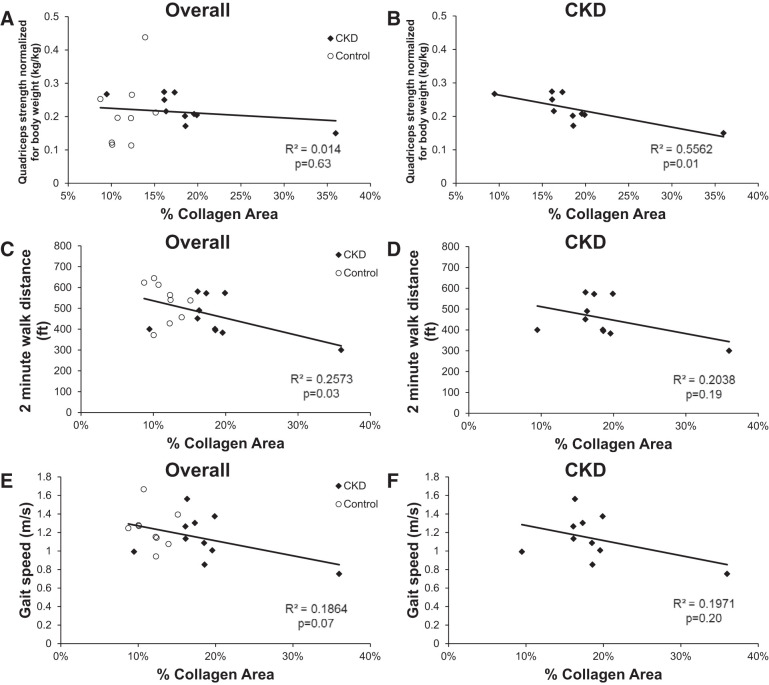
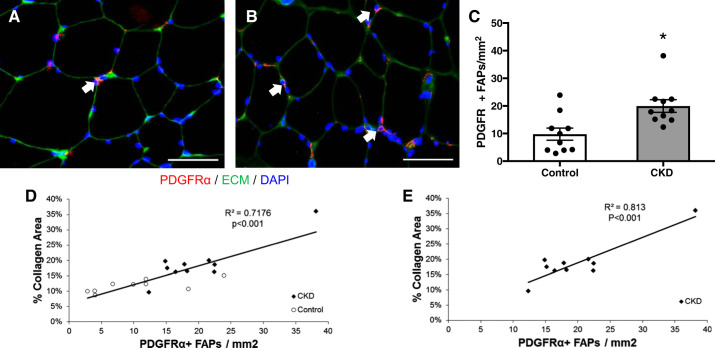
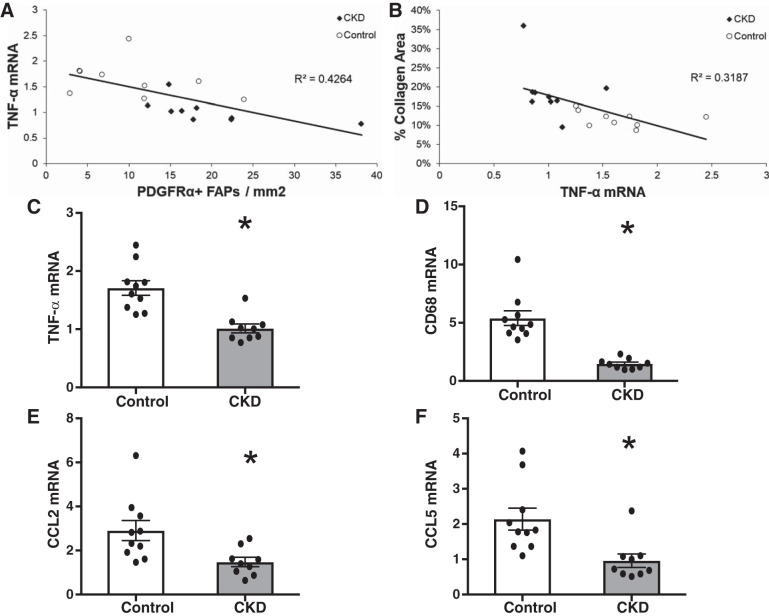
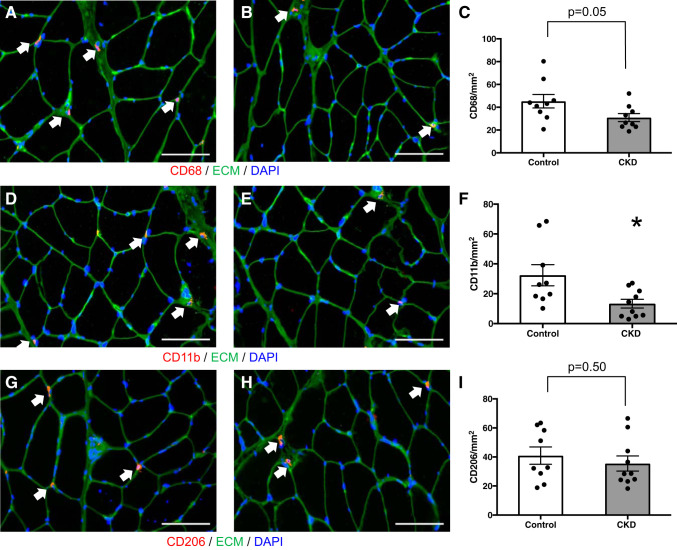
Muscle dysfunction is an important cause of morbidity among patients with chronic kidney disease (CKD). Although muscle fibrosis is present in a CKD rodent model, its existence in humans and its impact on physical function are currently unknown. We examined isometric leg extension strength and measures of skeletal muscle fibrosis and inflammation in vastus lateralis muscle from CKD patients ( n = 10) and healthy, sedentary controls ( n = 10). Histochemistry and immunohistochemistry were used to assess muscle collagen and macrophage and fibro/adipogenic progenitor (FAP) cell populations, and RT-qPCR was used to assess muscle-specific inflammatory marker expression. Muscle collagen content was significantly greater in CKD compared with control (18.8 ± 2.1 vs. 11.7 ± 0.7% collagen area, P = 0.008), as was staining for collagen I, pro-collagen I, and a novel collagen-hybridizing peptide that binds remodeling collagen. Muscle collagen was inversely associated with leg extension strength in CKD ( r = -0.74, P = 0.01). FAP abundance was increased in CKD, was highly correlated with muscle collagen ( r = 0.84, P < 0.001), and was inversely associated with TNF-α expression ( r = -0.65, P = 0.003). TNF-α, CD68, CCL2, and CCL5 mRNA were significantly lower in CKD than control, despite higher serum TNF-α and IL-6. Immunohistochemistry confirmed fewer CD68+ and CD11b+ macrophages in CKD muscle. In conclusion, skeletal muscle collagen content is increased in humans with CKD and is associated with functional parameters. Muscle fibrosis correlated with increased FAP abundance, which may be due to insufficient macrophage-mediated TNF-α secretion. These data provide a foundation for future research elucidating the mechanisms responsible for this newly identified human muscle pathology.
Keywords: chronic kidney disease; fibrosis; inflammation; skeletal muscle.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous