

Wearable Cardioverter-Defibrillator after Myocardial Infarction
- PMID: 30280654
- PMCID: PMC6276371
- DOI: 10.1056/NEJMoa1800781
Wearable Cardioverter-Defibrillator after Myocardial Infarction
Abstract
Background: Despite the high rate of sudden death after myocardial infarction among patients with a low ejection fraction, implantable cardioverter-defibrillators are contraindicated until 40 to 90 days after myocardial infarction. Whether a wearable cardioverter-defibrillator would reduce the incidence of sudden death during this high-risk period is unclear.
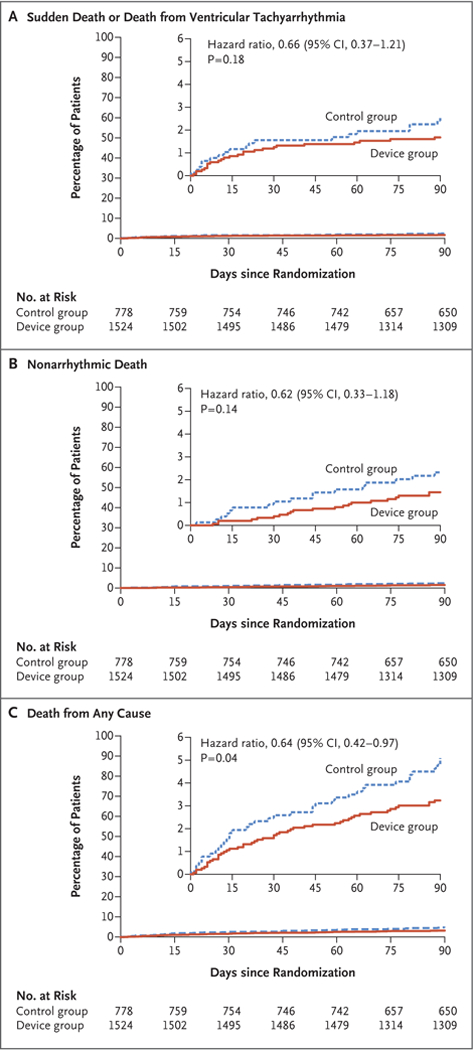
Methods: We randomly assigned (in a 2:1 ratio) patients with acute myocardial infarction and an ejection fraction of 35% or less to receive a wearable cardioverter-defibrillator plus guideline-directed therapy (the device group) or to receive only guideline-directed therapy (the control group). The primary outcome was the composite of sudden death or death from ventricular tachyarrhythmia at 90 days (arrhythmic death). Secondary outcomes included death from any cause and nonarrhythmic death.
Results: Of 2302 participants, 1524 were randomly assigned to the device group and 778 to the control group. Participants in the device group wore the device for a median of 18.0 hours per day (interquartile range, 3.8 to 22.7). Arrhythmic death occurred in 1.6% of the participants in the device group and in 2.4% of those in the control group (relative risk, 0.67; 95% confidence interval [CI], 0.37 to 1.21; P=0.18). Death from any cause occurred in 3.1% of the participants in the device group and in 4.9% of those in the control group (relative risk, 0.64; 95% CI, 0.43 to 0.98; uncorrected P=0.04), and nonarrhythmic death in 1.4% and 2.2%, respectively (relative risk, 0.63; 95% CI, 0.33 to 1.19; uncorrected P=0.15). Of the 48 participants in the device group who died, 12 were wearing the device at the time of death. A total of 20 participants in the device group (1.3%) received an appropriate shock, and 9 (0.6%) received an inappropriate shock.
Conclusions: Among patients with a recent myocardial infarction and an ejection fraction of 35% or less, the wearable cardioverter-defibrillator did not lead to a significantly lower rate of the primary outcome of arrhythmic death than control. (Funded by the National Institutes of Health and Zoll Medical; VEST ClinicalTrials.gov number, NCT01446965 .).
Figures
Comment in
-
Another Shock for Sudden Death Prevention after Myocardial Infarction.N Engl J Med. 2018 Sep 27;379(13):1274-1275. doi: 10.1056/NEJMe1809832. N Engl J Med. 2018. PMID: 30257160 No abstract available.
-
A wearable cardioverter-defibrillator did not reduce arrhythmic death in MI with reduced ejection fraction.Ann Intern Med. 2019 Jan 15;170(2):JC5. doi: 10.7326/ACPJC-2019-170-2-005. Ann Intern Med. 2019. PMID: 30641556 No abstract available.
-
Wearable Cardioverter–Defibrillator after Myocardial Infarction.N Engl J Med. 2019 Feb 7;380(6):599. doi: 10.1056/NEJMc1816889. N Engl J Med. 2019. PMID: 30730691 No abstract available.
-
Wearable Cardioverter–Defibrillator after Myocardial Infarction.N Engl J Med. 2019 Feb 7;380(6):600. doi: 10.1056/NEJMc1816889. N Engl J Med. 2019. PMID: 30730692 No abstract available.
References
-
- Berger CJ, Murabito JM, Evans JC, Anderson KM, Levy D. Prognosis after first myocardial infarction: comparison of Q-wave and non-Q-wave myocardial infarction in the Framingham Heart Study. JAMA 1992;268:1545–51. - PubMed
-
- Kannel WB, Sorlie P, McNamara PM. Prognosis after initial myocardial infarction: the Framingham study. Am J Cardiol 1979;44:53–9. - PubMed
-
- Solomon SD, Zelenkofske S, McMurray JJV, et al. Sudden death in patients with myocardial infarction and left ventricular dysfunction, heart failure, or both. N Engl J Med 2005;352:2581–8. - PubMed
-
- Julian DG, Camm AJ, Frangin G, et al. Randomised trial of effect of amiodarone on mortality in patients with left-ventricular dysfunction after recent myocardial infarction: EMIAT. Lancet 1997;349:667–74. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical