

Disease- and Treatment-related Morbidity in Adolescents With Perinatal HIV Infection in Asia
- PMID: 30281549
- PMCID: PMC6375771
- DOI: 10.1097/INF.0000000000002208
Disease- and Treatment-related Morbidity in Adolescents With Perinatal HIV Infection in Asia
Abstract
Background: Perinatally HIV-infected adolescents (PHIVA) are exposed to a chronic systemic infection and long-term antiretroviral therapy (ART), leaving them susceptible to morbidities associated with inflammation, immunodeficiency and drug toxicity.
Methods: Data collected 2001 to 2016 from PHIVA 10-19 years of age within a regional Asian cohort were analyzed using competing risk time-to-event and Poisson regression analyses to describe the nature and incidence of morbidity events and hospitalizations and identify factors associated with disease-related, treatment-related and overall morbidity. Morbidity was defined according to World Health Organization clinical staging criteria and U.S. National Institutes of Health Division of AIDS criteria.
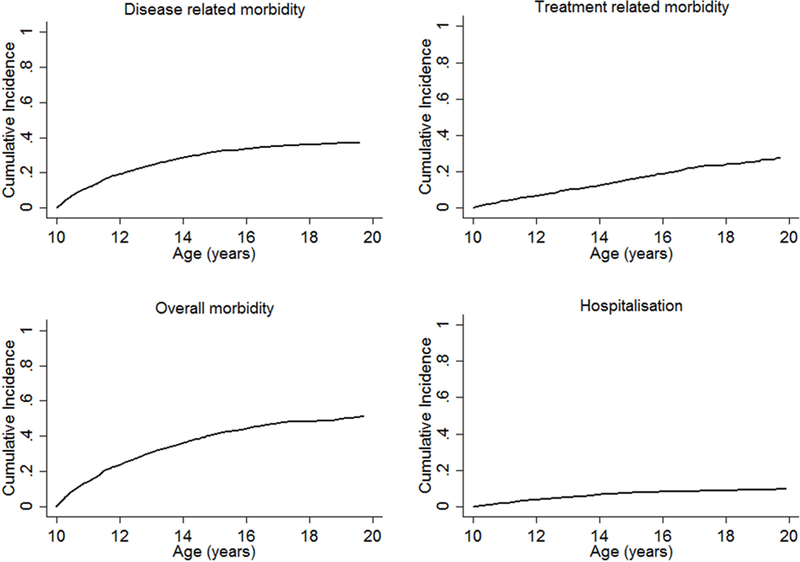
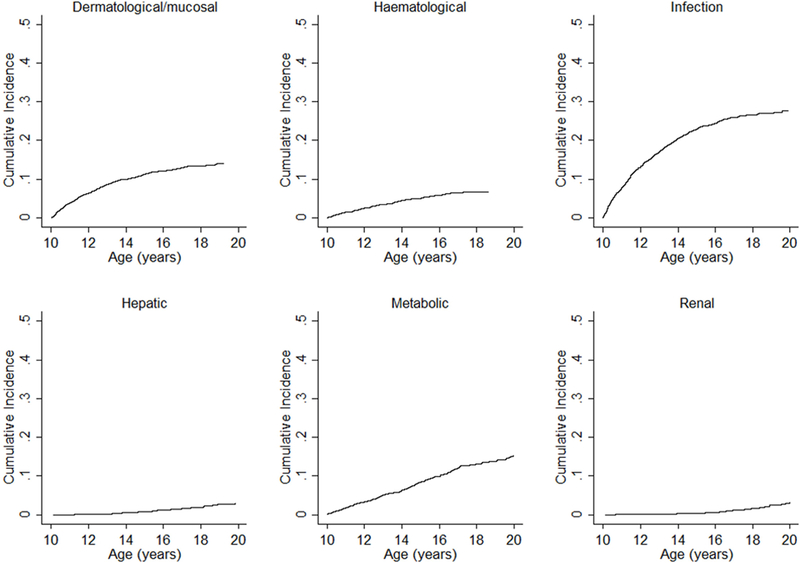
Results: A total 3,448 PHIVA contributed 17,778 person-years. Median age at HIV diagnosis was 5.5 years, and ART initiation was 6.9 years. There were 2,562 morbidity events and 307 hospitalizations. Cumulative incidence for any morbidity was 51.7%, and hospitalization was 10.0%. Early adolescence was dominated by disease-related infectious morbidity, with a trend toward noninfectious and treatment-related morbidity in later adolescence. Higher overall morbidity rates were associated with a CD4 count <350 cells/µL, HIV viral load ≥10,000 copies/mL and experiencing prior morbidity at age <10 years. Lower overall morbidity rates were found for those 15-19 years of age compared with 10-14 years and those who initiated ART at age 5-9 years compared with <5 or ≥10 years.
Conclusions: Half of our PHIVA cohort experienced a morbidity event, with a trend from disease-related infectious events to treatment-related and noninfectious events as PHIVA age. ART initiation to prevent immune system damage, optimize virologic control and minimize childhood morbidity are key to limiting adolescent morbidity.
Conflict of interest statement
AHS has received travel and grant support to her institution from ViiV Healthcare. Other authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The TREAT Asia Pediatric HIV Observational Database is an initiative of TREAT Asia, a program of amfAR, The Foundation for AIDS Research, with support from the U.S. National Institutes of Health’s National Institute of Allergy and Infectious Diseases, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Cancer Institute, National Institute of Mental Health, and National Institute on Drug Abuse as part of the International Epidemiology Databases to Evaluate AIDS (IeDEA; U01AI069907). The Kirby Institute is funded by the Australian Government Department of Health and Ageing, and is affiliated with the Faculty of Medicine, UNSW Australia. AWB received support from an Australian Government Research Training Program Scholarship. The content of this publication is solely the responsibility of the authors and does not necessarily represent the official views of any of the governments or institutions mentioned above.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
