

Cardiovascular disease and COPD: dangerous liaisons?
- PMID: 30282634
- PMCID: PMC9488649
- DOI: 10.1183/16000617.0057-2018
Cardiovascular disease and COPD: dangerous liaisons?
Erratum in
-
"Cardiovascular disease and COPD: dangerous liaisons." Klaus F. Rabe, John R. Hurst and Samy Suissa. Eur Respir Rev 2018; 27: 180057.Eur Respir Rev. 2018 Nov 21;27(150):185057. doi: 10.1183/16000617.5057-2018. Print 2018 Dec 31. Eur Respir Rev. 2018. PMID: 30463874 Free PMC article. No abstract available.
Abstract
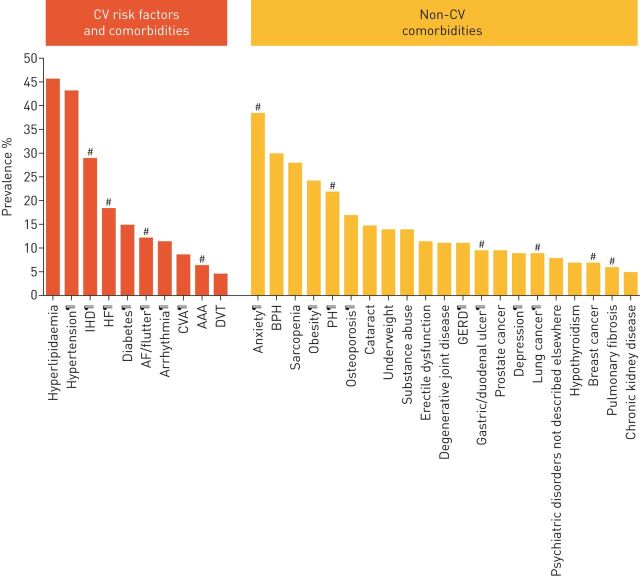
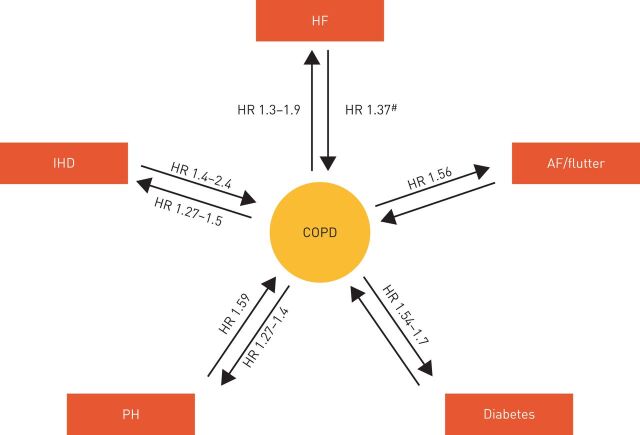
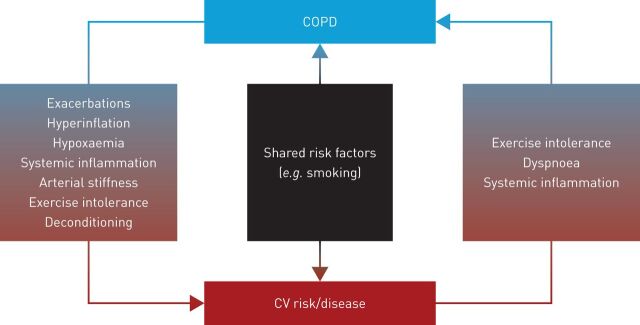
Chronic obstructive pulmonary disease (COPD) and cardiovascular disease (CVD) frequently occur together and their coexistence is associated with worse outcomes than either condition alone. Pathophysiological links between COPD and CVD include lung hyperinflation, systemic inflammation and COPD exacerbations. COPD treatments may produce beneficial cardiovascular (CV) effects, such as long-acting bronchodilators, which are associated with improvements in arterial stiffness, pulmonary vasoconstriction, and cardiac function. However, data are limited regarding whether these translate into benefits in CV outcomes. Some studies have suggested that treatment with long-acting β2-agonists and long-acting muscarinic antagonists leads to an increase in the risk of CV events, particularly at treatment initiation, although the safety profile of these agents with prolonged use appears reassuring. Some CV medications may have a beneficial impact on COPD outcomes, but there have been concerns about β-blocker use leading to bronchospasm in COPD, which may result in patients not receiving guideline-recommended treatment. However, there are few data suggesting harm with these agents and patients should not be denied β-blockers if required. Clearer recommendations are necessary regarding the identification and management of comorbid CVD in patients with COPD in order to facilitate early intervention and appropriate treatment.
Copyright ©ERS 2018.
Conflict of interest statement
Conflict of interest: K.F. Rabe reports personal fees (consultant and speakers fees) from AstraZeneca, Boehringer Ingelheim, Novartis, Sanofi, Teva, Intermune, Chiesi Pharmaceuticals and Berlin Chemie, as well as grants from the Ministry of Education and Science, Germany, outside the submitted work. Conflict of interest: J. Hurst reports grants, personal fees and non-financial support from pharmaceutical companies that make medicines to treat COPD, outside the submitted work. Conflict of interest: S. Suissa reports grants and personal fees (board membership and research grant) from Novartis and Boehringer Ingelheim, and personal fees (lectures) from AstraZeneca, outside the submitted work.
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) . Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2018 report). https://goldcopd.org/wp-content/uploads/2017/11/GOLD-2018-v6.0-FINAL-rev... Date last accessed: November 28, 2017.
-
- Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2012; 186: 155–161. - PubMed
-
- van den Akker M, Buntinx F, Knottnerus JA. Comorbidity or multimorbidity: what's in a name? A review of literature. Eur J Gen Pract 1996; 2: 65–70.
-
- Bhatt SP, Dransfield MT. AECOPD: acute exacerbations of chronic obstructive cardiopulmonary disease? Am J Respir Crit Care Med 2013; 188: 1046–1048. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical