

Reduced prevalence of small-for-gestational-age and preterm birth for women of low socioeconomic position: a population-based cohort study comparing antenatal midwifery and physician models of care
- PMID: 30282682
- PMCID: PMC6169769
- DOI: 10.1136/bmjopen-2018-022220
Reduced prevalence of small-for-gestational-age and preterm birth for women of low socioeconomic position: a population-based cohort study comparing antenatal midwifery and physician models of care
Abstract
Objective: Our aim was to investigate if antenatal midwifery care was associated with lower odds of small-for-gestational-age (SGA) birth, preterm birth (PTB) or low birth weight (LBW) compared with general practitioner (GP) or obstetrician (OB) models of care for women of low socioeconomic position.
Setting: This population-level, retrospective cohort study used province-wide maternity, medical billing and demographic data from British Columbia, Canada.
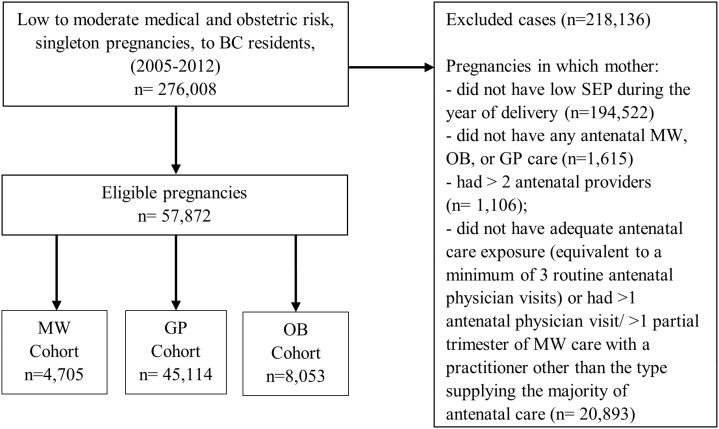
Participants: Our study included 57 872 pregnant women, with low socioeconomic position, who: were residents of British Columbia, Canada, carried a singleton fetus, had low to moderate medical/obstetric risk, delivered between 2005 and 2012 and received medical insurance premium assistance.
Primary and secondary outcome measures: We report rates, adjusted ORs (aOR), and 95% CIs for the primary outcome, SGA birth (<the 10th percentile), and secondary outcomes, PTB (<37 weeks' completed gestation) and LBW (<2500 g).
Results: Our sample included 4705 midwifery patients, 45 114 GP patients and 8053 OB patients. Odds of SGA birth were reduced for patients receiving antenatal midwifery versus GP (aOR 0.71, 95% CI 0.62 to 0.82) or OB care (aOR 0.59, 95% CI 0.50 to 0.69). Odds of PTB were lower for antenatal midwifery versus GP (aOR 0.74, 95% CI 0.63 to 0.86) or OB patients (aOR 0.53, 95% CI 0.45 to 0.62). Odds of LBW were reduced for midwifery versus GP (aOR 0.66, 95% CI 0.53 to 0.82) or OB patients (aOR 0.43, 95% CI 0.34 to 0.54).
Conclusion: Antenatal midwifery care in British Columbia, Canada, was associated with lower odds of SGA birth, PTB and LBW, for women of low socioeconomic position, compared with physician models of care. Results support the development of policy to ensure antenatal midwifery care is available and accessible for women of low socioeconomic position. Future research is needed to determine the underlying mechanisms linking midwifery care to better birth outcomes for women of low socioeconomic position.
Keywords: birth outcomes; fetal medicine; maternal medicine; midwifery; quality in healthcare; socioeconomic status.
© Author(s) (or their employer(s)) 2018. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: As of May 2018, DNM has been providing consulting services to the Midwives Association of BC. No other authors have competing interests to declare.
Figures
References
-
- Heins HC, Nance NW, McCarthy BJ, et al. A randomized trial of nurse-midwifery prenatal care to reduce low birth weight. Obstet Gynecol 1990;75(3 Pt 1):341–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous