

Paraneoplastic neuronal intermediate filament autoimmunity
- PMID: 30282771
- PMCID: PMC6207411
- DOI: 10.1212/WNL.0000000000006435
Paraneoplastic neuronal intermediate filament autoimmunity
Abstract
Objective: To describe paraneoplastic neuronal intermediate filament (NIF) autoimmunity.
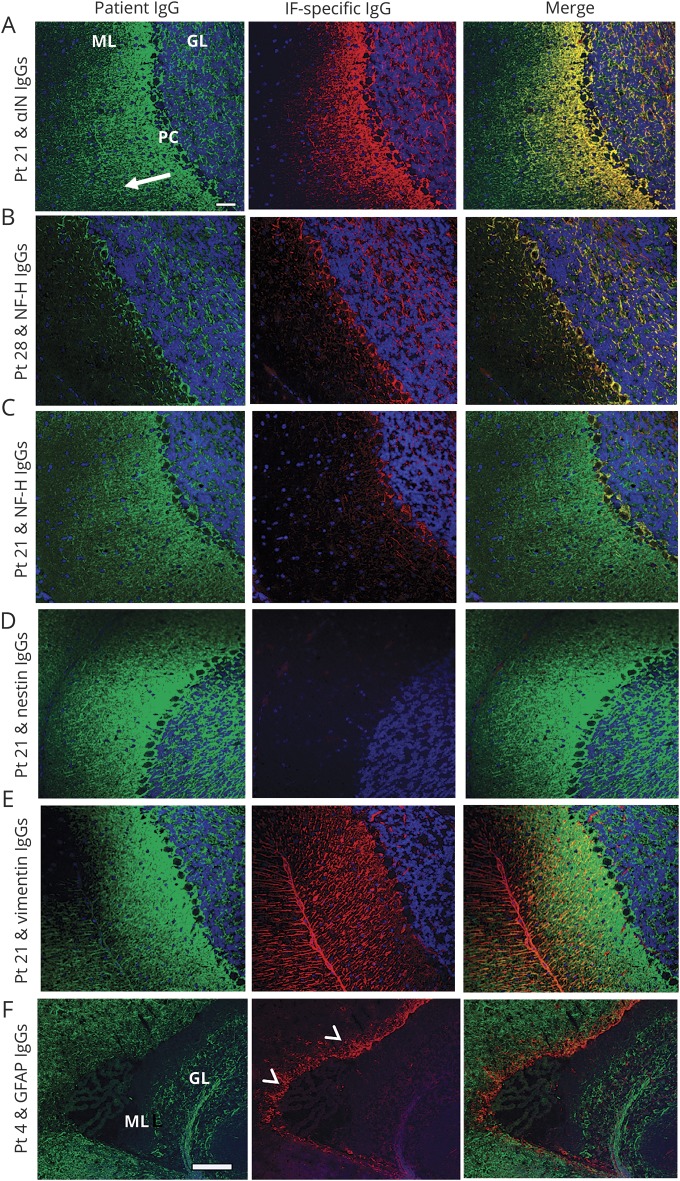
Methods: Archived patient and control serum and CSF specimens were evaluated by tissue-based indirect immunofluorescence assay (IFA). Autoantigens were identified by Western blot and mass spectrometry. NIF specificity was confirmed by dual tissue section staining and 5 recombinant NIF-specific HEK293 cell-based assays (CBAs, for α-internexin, neurofilament light [NfL], neurofilament medium, or neurofilament heavy chain, and peripherin). NIF-immunoglobulin Gs (IgGs) were correlated with neurologic syndromes and cancers.
Results: Among 65 patients, NIF-IgG-positive by IFA and CBAs, 33 were female (51%). Median symptom onset age was 62 years (range 18-88). Patients fell into 2 groups, defined by the presence of NfL-IgG (21 patients, who mostly had ≥4 NIF-IgGs detected) or its absence (44 patients, who mostly had ≤2 NIF-IgGs detected). Among NfL-IgG-positive patients, 19/21 had ≥1 subacute onset CNS disorders: cerebellar ataxia (11), encephalopathy (11), or myelopathy (2). Cancers were detected in 16 of 21 patients (77%): carcinomas of neuroendocrine lineage (10) being most common (small cell [5], Merkel cell [3], other neuroendocrine [2]). Two of 257 controls (0.8%, both with small cell carcinoma) were positive by both IFA and CBA. Five of 7 patients with immunotherapy data improved. By comparison, the 44 NfL-IgG-negative patients had findings of unclear significance: diverse nervous system disorders (p = 0.006), as well as limited (p = 0.003) and more diverse (p < 0.0001) cancer accompaniments.
Conclusions: NIF-IgG detection by IFA, with confirmatory CBA testing that yields a profile including NfL-IgG, defines a paraneoplastic CNS disorder (usually ataxia or encephalopathy) accompanying neuroendocrine lineage neoplasia.
Copyright © 2018 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures





References
-
- McKeon A, Pittock SJ. Paraneoplastic encephalomyelopathies: pathology and mechanisms. Acta Neuropathol 2011;122:381–400. - PubMed
-
- Fang B, McKeon A, Hinson SR, et al. Autoimmune glial fibrillary acidic protein astrocytopathy: a novel meningoencephalomyelitis. JAMA Neurol 2016;73:1297–1307. - PubMed
-
- Flanagan EP, Hinson SR, Lennon VA, et al. Glial fibrillary acidic protein immunoglobulin G as biomarker of autoimmune astrocytopathy: analysis of 102 patients. Ann Neurol 2017;81:298–309. - PubMed
-
- Braxton DB, Williams M, Kamali D, Chin S, Liem R, Latov N. Specificity of human anti-neurofilament autoantibodies. J Neuroimmunol 1989;21:193–203. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources