Caudal Analgesia for Hypospadias in Pediatrics: Comparative Evaluation of Adjuvants Dexamethasone and Dexmedetomidine Combination versus Dexamethasone or Dexmedetomidine to Bupivacaine: A Prospective, Double-Blinded, Randomized Comparative Study
- PMID: 30283169
- PMCID: PMC6157238
- DOI: 10.4103/aer.AER_77_18
Caudal Analgesia for Hypospadias in Pediatrics: Comparative Evaluation of Adjuvants Dexamethasone and Dexmedetomidine Combination versus Dexamethasone or Dexmedetomidine to Bupivacaine: A Prospective, Double-Blinded, Randomized Comparative Study
Abstract
Background: Caudal block is the most commonly used regional anesthetic technique in pediatric surgeries; different additives have been used for better and safer outcome.
Aim: The aim of this study is to compare the combination of dexamethasone and dexmedetomidine as adjuvants to bupivacaine versus using each agent solely with bupivacaine in pediatric caudal block as regards their efficiency in pain relief (the duration of postoperative analgesia, first time to request analgesia, and modified objective pain score [MOPS]).
Study design: This was a prospective, double-blinded, randomized study.
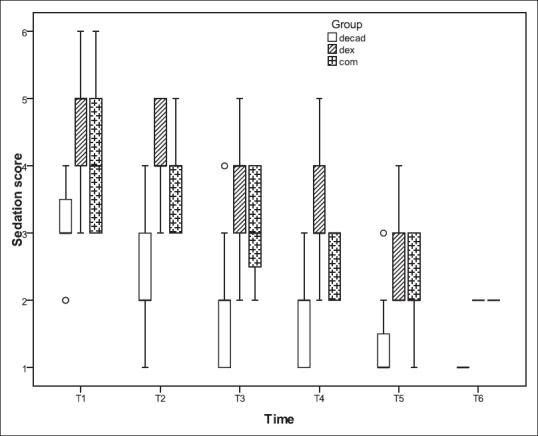
Patients and methods: Patients and Methods: Sixty-three children scheduled for hypospadias surgery wererandomized into three groupsaccording to the adjuvant drug added to caudal bupivacaine : Group I (n = 21): dexamethasone 0.1 mg/kg + 0.5 mg/kg bupivacaine 0.25%, Group II (n = 21): dexmedetomidine0.01 μg/kg + 0.5 mg/kg bupivacaine 0.25% and Group III (n = 21): dexamethasone 0.1 mg/kg + dexmedetomidine 0.01 μg/kg + 0.5 mg/kgbupivacaine 0.25%. Intraoperative and postoperative hemodynamics were recorded. In postoperative anesthesia care unit and then the ward, MOPS and sedation score were recorded at 30 min and 1, 2, 3, 6 and 12 h. Further, the time of first analgesic request and side effects were recorded.
Statistical analysis: Categorical data were presented as frequencies (%) and analyzed using Chi-square test. Continuous data were presented as mean (standard deviation) and median (quartiles). Continuous data were analyzed using one-way analysis of variance for single measures and two-way mixed model for repeated measures. Kaplan-Meier analysis was performed for the duration of analgesia.
Results: In Group III, MOPS was lower than Groups I and II at the study times. Further, Group III had prolonged time for first request of analgesic. Sedation scores were prolonged in Group III and Group II than in Group I. There was a reduction in heart rates in Group III more than Group I and Group II but with no significant difference. However, there was a significant reduction in mean arterial blood pressure 30 min intraoperatively and postoperatively in Group III as compared to Groups I and II.
Conclusion: The addition of combined dexmedetomidine at a dose of 1 μg/kg and dexamethasone 0.1 mg/kg to caudal bupivacaine seemed to be an attractive alternative to each drug if used alone with more prolonged analgesia and almost no adverse effects.
Keywords: Caudal block; combined dexamethasone and dexmedetomidine; hypospadias surgery; pediatric surgery; postoperative analgesia.
Conflict of interest statement
There are no conflicts of interest.
Figures




Similar articles
-
Efficacy and safety of dexmedetomidine added to caudal bupivacaine in pediatric major abdominal cancer surgery.Pain Physician. 2014 Sep-Oct;17(5):393-400. Pain Physician. 2014. PMID: 25247897 Clinical Trial.
-
Dexmedetomidine as an adjuvant to bupivacaine in caudal analgesia in children.Anesth Essays Res. 2016 May-Aug;10(2):227-32. doi: 10.4103/0259-1162.174468. Anesth Essays Res. 2016. PMID: 27212752 Free PMC article.
-
Comparison of caudal bupivacaine alone with bupivacaine plus two doses of dexmedetomidine for postoperative analgesia in pediatric patients undergoing infra-umbilical surgery: a randomized controlled double-blinded study.Paediatr Anaesth. 2015 Sep;25(9):883-90. doi: 10.1111/pan.12686. Epub 2015 Jun 1. Paediatr Anaesth. 2015. PMID: 26033312 Clinical Trial.
-
Comparison of adjuvant pharmaceuticals for caudal block in pediatric lower abdominal and urological surgeries: A network meta-analysis.J Clin Anesth. 2022 Oct;81:110907. doi: 10.1016/j.jclinane.2022.110907. Epub 2022 Jun 18. J Clin Anesth. 2022. PMID: 35728381 Review.
-
Efficacy and safety of caudal dexmedetomidine in pediatric infra-umbilical surgery: a meta-analysis and trial-sequential analysis of randomized controlled trials.Reg Anesth Pain Med. 2021 May;46(5):422-432. doi: 10.1136/rapm-2020-102024. Epub 2021 Jan 15. Reg Anesth Pain Med. 2021. PMID: 33452203 Review.
Cited by
-
Adductor Canal Block Duration of Analgesia Successfully Prolonged With Perineural Dexmedetomidine and Dexamethasone in Addition to IPACK Block for Total Knee Arthroplasty.Cureus. 2020 Sep 21;12(9):e10566. doi: 10.7759/cureus.10566. Cureus. 2020. PMID: 33101812 Free PMC article.
-
Peripheral Nerve Blockade for Medial Patellofemoral Ligament Reconstruction in Pediatric Patients: The Addition of a Proximal Single-Injection Sciatic Nerve Block Provides Improved Analgesia.Local Reg Anesth. 2022 Jun 27;15:31-43. doi: 10.2147/LRA.S360738. eCollection 2022. Local Reg Anesth. 2022. PMID: 35782524 Free PMC article.
-
Guidelines for Opioid Prescribing in Children and Adolescents After Surgery: An Expert Panel Opinion.JAMA Surg. 2021 Jan 1;156(1):76-90. doi: 10.1001/jamasurg.2020.5045. JAMA Surg. 2021. PMID: 33175130 Free PMC article. Review.
-
Comparison of ultrasound-guided sacral erector spinae plane block and caudal epidural block for analgesia in paediatric patients undergoing hypospadias repair: A double-blind, randomised controlled trial.Indian J Anaesth. 2024 Aug;68(8):725-730. doi: 10.4103/ija.ija_13_24. Epub 2024 Jul 2. Indian J Anaesth. 2024. PMID: 39176123 Free PMC article.
-
Optimizing Paediatric Hypospadias Surgical Repair: Pudendal Nerve Block Versus Caudal Block for Superior Analgesia.Turk J Anaesthesiol Reanim. 2025 May 30;53(3):114-121. doi: 10.4274/TJAR.2025.241773. Epub 2025 Apr 9. Turk J Anaesthesiol Reanim. 2025. PMID: 40200590 Free PMC article.
References
-
- Ansermino M, Basu R, Vandebeek C, Montgomery C. Nonopioid additives to local anaesthetics for caudal blockade in children: A systematic review. Paediatr Anaesth. 2003;13:561–73. - PubMed
-
- Engelman E, Marsala C. Bayesian enhanced meta-analysis of post-operative analgesic efficacy of additives for caudal analgesia in children. Acta Anaesthesiol Scand. 2012;56:817–32. - PubMed
-
- De Oliveira GS, Jr, Almeida MD, Benzon HT, McCarthy RJ. Perioperative single dose systemic dexamethasone for postoperative pain: A meta-analysis of randomized controlled trials. Anesthesiology. 2011;115:575–88. - PubMed