

Functional Anatomy of the Inferior Longitudinal Fasciculus: From Historical Reports to Current Hypotheses
- PMID: 30283306
- PMCID: PMC6156142
- DOI: 10.3389/fnana.2018.00077
Functional Anatomy of the Inferior Longitudinal Fasciculus: From Historical Reports to Current Hypotheses
Abstract
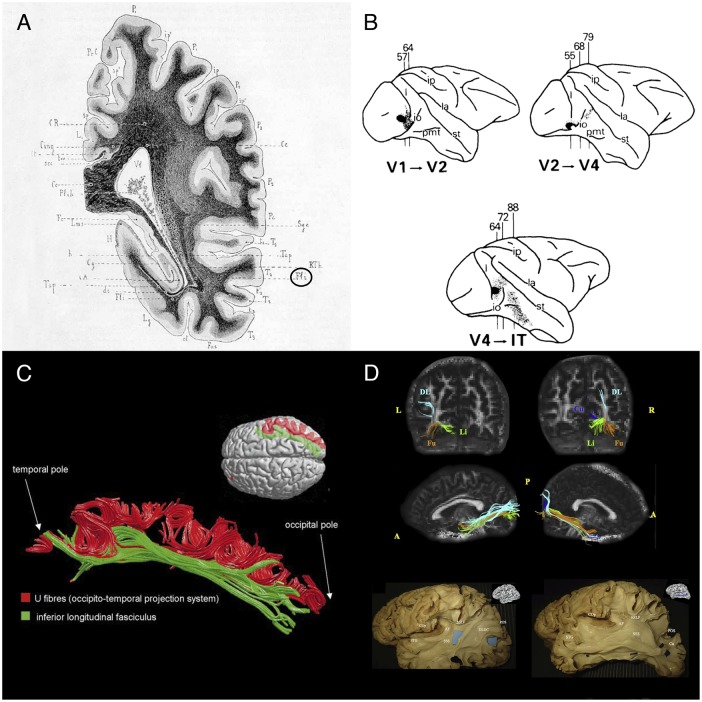
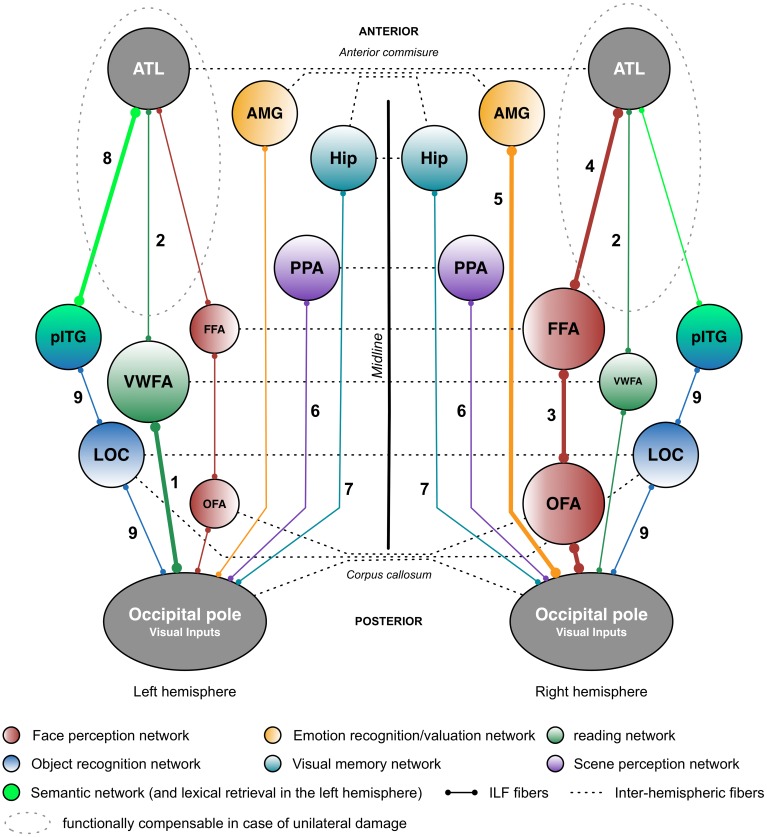
The inferior longitudinal fasciculus (ILF) is a long-range, associative white matter pathway that connects the occipital and temporal-occipital areas of the brain to the anterior temporal areas. In view of the ILF's anatomic connections, it has been suggested that this pathway has a major role in a relatively large array of brain functions. Until recently, however, the literature data on these potential functions were scarce. Here, we review the key findings of recent anatomic, neuromodulation, and neuropsychological studies. We also summarize reports on how this tract is disrupted in a wide range of brain disorders, including psychopathologic, neurodevelopmental, and neurologic diseases. Our review reveals that the ILF is a multilayered, bidirectional tract involved in processing and modulating visual cues and thus in visually guided decisions and behaviors. Accordingly, sudden disruption of the ILF by neurologic insult is mainly associated with neuropsychological impairments of visual cognition (e.g., visual agnosia, prosopagnosia, and alexia). Furthermore, disruption of the ILF may constitute the pathophysiologic basis for visual hallucinations and socio-emotional impairments in schizophrenia, as well as emotional difficulties in autism spectrum disorder. Degeneration of the ILF in neurodegenerative diseases affecting the temporal lobe may explain (at least in part) the gradual onset of semantic and lexical access difficulties. Although some of the functions mediated by the ILF appear to be relatively lateralized, observations from neurosurgery suggest that disruption of the tract's anterior portion can be dynamically compensated for by the contralateral portion. This might explain why bilateral disruption of the ILF in either acute or progressive disease is highly detrimental in neuropsychological terms.
Keywords: emotion recognition; inferior longitudinal fasciculus; lexical retrieval; prosopagnosia; reading; semantics; ventral pathway; visual agnosia.
Figures
References
-
- Albert M. L., Soffer D., Silverberg R., Reches A. (1979). The anatomic basis of visual agnosia. Neurology 29 876–876. - PubMed
Publication types
LinkOut - more resources
Full Text Sources