

Rifaximin has the potential to prevent complications of cirrhosis
- PMID: 30283499
- PMCID: PMC6166307
- DOI: 10.1177/1756284818800307
Rifaximin has the potential to prevent complications of cirrhosis
Abstract
Background: Cirrhosis-related complications are associated with poor prognosis. With our analyses, we examined the potential benefit of rifaximin in reducing the risk of developing cirrhosis-related complications.
Methods: Adults with cirrhosis and hepatic encephalopathy (HE) in remission were randomly assigned to receive rifaximin 550 mg twice daily or placebo for 6 months with concomitant lactulose permitted. Post hoc analyses examined time to cirrhosis-related complications (HE, spontaneous bacterial peritonitis (SBP), variceal bleeding, acute kidney injury/hepatorenal syndrome). Subgroup analyses evaluated efficacy for select baseline disease characteristics.
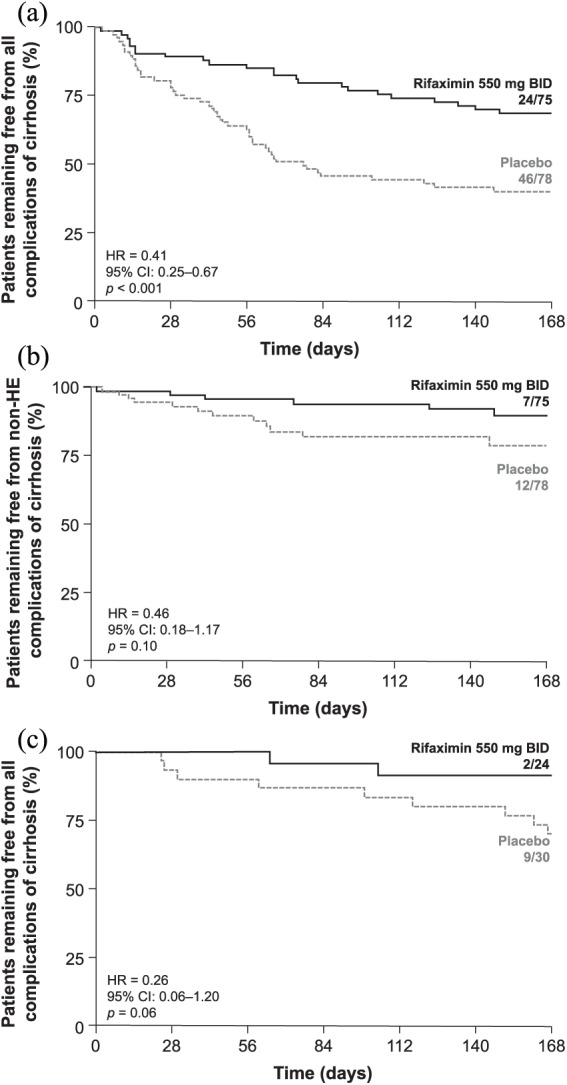
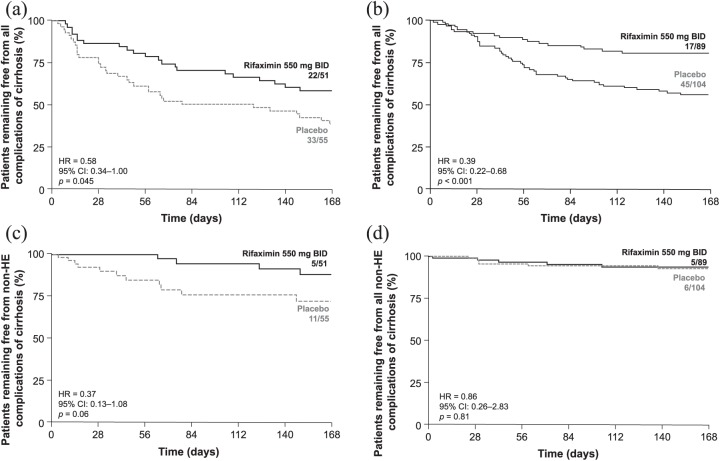
Results: Of patients receiving rifaximin (n = 140) and placebo (n = 159), 53.6% and 49.1%, respectively, had baseline Model for End-Stage Liver Disease (MELD) score ⩾ 12 and international normalized ratio (INR) ⩾ 1.2. Baseline ascites was observed in 36.4% (rifaximin) and 34.6% (placebo) of patients. In patients with MELD score ⩾ 12 and INR ⩾ 1.2, rifaximin reduced the relative risk (RR) of any first complication experienced during trial by 59% [hazard ratio (HR) = 0.41, 95% confidence interval (CI): 0.25-0.67; p < 0.001] versus placebo. For patients with baseline ascites, rifaximin reduced the RR of any first complication experienced during trial by 42% versus placebo (HR = 0.58, 95% CI: 0.34-1.0; p = 0.045). For some subgroups, there was a decrease in RR of complications of SBP, variceal bleeding, and acute kidney injury/hepatorenal syndrome with rifaximin versus placebo, although there were few events reported in the study.
Conclusion: Rifaximin may reduce the incidence of cirrhosis-related complications and the recurrence of overt HE.[ClinicalTrials.gov identifier: NCT00298038.].
Keywords: antibiotic; cirrhosis; decompensation; hepatic encephalopathy; rifaximin.
Conflict of interest statement
Conflict of interest statement: SL Flamm is a consultant and has served on the speakers’ bureau for AbbVie, Gilead Sciences, Inc., Intercept Pharmaceuticals, Inc., Merck & Co., Inc., and Salix Pharmaceuticals; and has received research support from AbbVie, Gilead Sciences, Inc., and Intercept Pharmaceuticals, Inc. KD Mullen has served as a consultant for Salix Pharmaceuticals and Norgine. Z Heimanson is an employee of Salix Pharmaceuticals. AJ Sanyal has stock options in Genfit and is the president of Sanyal Biotechnology. He has served as a consultant to AbbVie, AstraZeneca, Bristol-Myers Squibb Company, DURECT Corporation, Enanta Pharmaceuticals, Inc., Galmed Pharmaceuticals Ltd., Genfit, Gilead Sciences, Inc., Ikaria, Immuron, Intercept Pharmaceuticals, Inc., Eli Lilly and Company, Merck & Co., Inc., Nitto Denko Corporation, Novartis, Salix Pharmaceuticals, and Zafgen.
Figures
References
-
- Ginés P, Quintero E, Arroyo V, et al. Compensated cirrhosis: natural history and prognostic factors. Hepatology 1987; 7: 122–128. - PubMed
-
- D’Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol 2006; 44: 217–231. - PubMed
-
- Starr SP, Raines D. Cirrhosis: diagnosis, management, and prevention. Am Fam Physician 2011; 84: 1353–1359. - PubMed
-
- Garcia-Tsao G, Lim JK; Members of the Veterans Affairs Hepatitis C Resource Center Program. Management and treatment of patients with cirrhosis and portal hypertension: recommendations from the Department of Veterans Affairs Hepatitis C Resource Center Program and the National Hepatitis C Program. Am J Gastroenterol 2009; 104: 1802–1829. - PubMed
-
- Landis CS, Ghabril M, Rustgi V, et al. Prospective multicenter observational study of overt hepatic encephalopathy. Dig Dis Sci 2016; 61: 1728–1734. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
