

Randomised controlled trial comparing modified Sano's and narrow band imaging international colorectal endoscopic classifications for colorectal lesions
- PMID: 30283604
- PMCID: PMC6162252
- DOI: 10.4253/wjge.v10.i9.210
Randomised controlled trial comparing modified Sano's and narrow band imaging international colorectal endoscopic classifications for colorectal lesions
Abstract
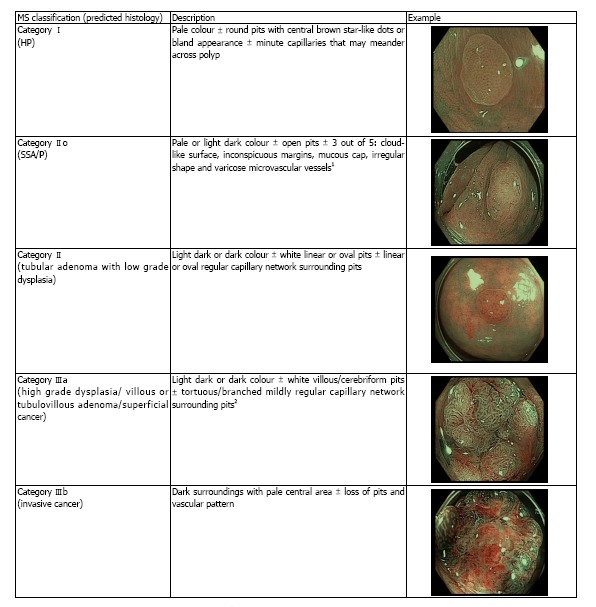
Aim: To assess the utility of modified Sano's (MS) vs the narrow band imaging international colorectal endoscopic (NICE) classification in differentiating colorectal polyps.
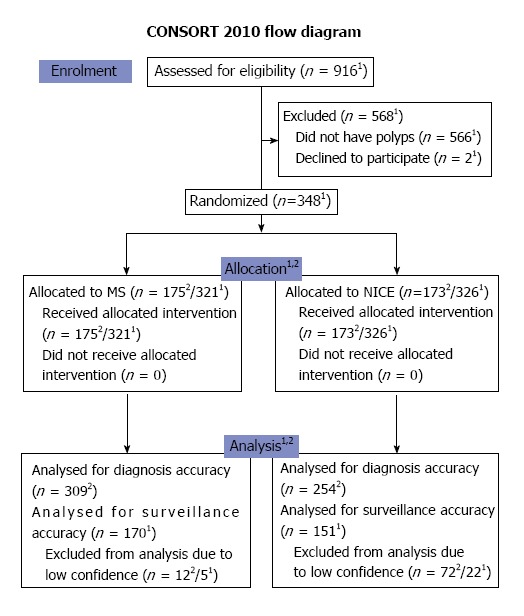
Methods: Patients undergoing colonoscopy between 2013 and 2015 were enrolled in this trial. Based on the MS or the NICE classifications, patients were randomised for real-time endoscopic diagnosis. This was followed by biopsies, endoscopic or surgical resection. The endoscopic diagnosis was then compared to the final (blinded) histopathology. The primary endpoint was the sensitivity (Sn), specificity (Sp), positive predictive value (PPV) and negative predictive value (NPV) of differentiating neoplastic and non-neoplastic polyps (MS II/IIo / IIIa / IIIb vs I or NICE 1 vs 2/3). The secondary endpoints were "endoscopic resectability" (MS II/IIo/IIIa vs I/IIIb or NICE 2 vs 1/3), NPV for diminutive distal adenomas and prediction of post-polypectomy surveillance intervals.
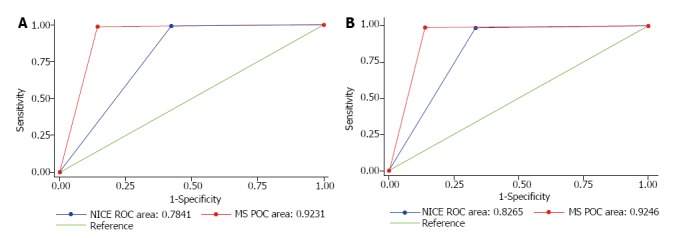
Results: A total of 348 patients were evaluated. The Sn, Sp, PPV and NPV in differentiating neoplastic polyps from non-neoplastic polyps were, 98.9%, 85.7%, 98.2% and 90.9% for MS; and 99.1%, 57.7%, 95.4% and 88.2% for NICE, respectively. The area under the receiver operating characteristic curve (AUC) for MS was 0.92 (95%CI: 0.86-0.98); and AUC for NICE was 0.78 (95%CI: 0.69, 0.88). The Sn, Sp, PPV and NPV in predicting "endoscopic resectability" were 98.9%, 86.1%, 97.8% and 92.5% for MS; and 98.6%, 66.7%, 94.7% and 88.9% for NICE, respectively. The AUC for MS was 0.92 (95%CI: 0.87-0.98); and the AUC for NICE was 0.83 (95%CI: 0.75-0.90). The AUC values were statistically different for both comparisons (P = 0.0165 and P = 0.0420, respectively). The accuracy for diagnosis of sessile serrated adenoma/polyp (SSA/P) with high confidence utilizing MS classification was 93.2%. The differentiation of SSA/P from other lesions achieved Sp, Sn, PPV and NPV of 87.2%, 91.5%, 89.6% and 98.6%, respectively. The NPV for predicting adenomas in diminutive rectosigmoid polyps (n = 150) was 96.6% and 95% with MS and NICE respectively. The calculated accuracy of post-polypectomy surveillance for MS group was 98.2% (167 out of 170) and for NICE group was 92.1% (139 out of 151).
Conclusion: The MS classification outperformed the NICE classification in differentiating neoplastic polyps and predicting endoscopic resectability. Both classifications met ASGE PIVI thresholds.
Keywords: Colonoscopy; Colorectal adenomas; Colorectal lesions; Colorectal neoplasm; Colorectal polyps; Endoscopic imaging; Magnifying colonoscopy; Randomised controlled trial.
Conflict of interest statement
Conflict-of-interest statement: All the authors declare that they have no competing interests.
Figures
Similar articles
-
Narrow-band imaging with dual focus magnification in differentiating colorectal neoplasia.Dig Endosc. 2013 May;25 Suppl 2:16-20. doi: 10.1111/den.12075. Dig Endosc. 2013. PMID: 23617643
-
Narrow-band Imaging International Colorectal Endoscopic Classification to predict polyp histology: REDEFINE study (with videos).Gastrointest Endosc. 2016 Sep;84(3):479-486.e3. doi: 10.1016/j.gie.2016.02.020. Epub 2016 Feb 27. Gastrointest Endosc. 2016. PMID: 26928372
-
Accuracy of narrow-band imaging in predicting colonoscopy surveillance intervals and histology of distal diminutive polyps: results from a multicenter, prospective trial.Gastrointest Endosc. 2013 Jul;78(1):106-14. doi: 10.1016/j.gie.2013.01.035. Epub 2013 Apr 11. Gastrointest Endosc. 2013. PMID: 23582472 Clinical Trial.
-
Narrow band imaging to differentiate neoplastic and non-neoplastic colorectal polyps in real time: a meta-analysis of diagnostic operating characteristics.Gut. 2013 Dec;62(12):1704-13. doi: 10.1136/gutjnl-2012-303965. Epub 2013 Jan 7. Gut. 2013. PMID: 23300139 Free PMC article.
-
Endoscopic diagnosis of sessile serrated adenoma/polyp with and without dysplasia/carcinoma.World J Gastroenterol. 2018 Aug 7;24(29):3250-3259. doi: 10.3748/wjg.v24.i29.3250. World J Gastroenterol. 2018. PMID: 30090005 Free PMC article. Review.
Cited by
-
Accuracy and inter-observer agreement of the nice and kudo classifications of superficial colonic lesions: a comparative study.Int J Colorectal Dis. 2021 Jul;36(7):1561-1568. doi: 10.1007/s00384-021-03897-8. Epub 2021 Mar 1. Int J Colorectal Dis. 2021. PMID: 33649902
-
JAG consensus statements for training and certification in flexible sigmoidoscopy.Frontline Gastroenterol. 2023 Jan 27;14(3):181-200. doi: 10.1136/flgastro-2022-102259. eCollection 2023. Frontline Gastroenterol. 2023. PMID: 37056324 Free PMC article.
-
Comparison of different virtual chromoendoscopy classification systems for the characterization of colorectal lesions.JGH Open. 2020 Jul 7;4(5):818-826. doi: 10.1002/jgh3.12382. eCollection 2020 Oct. JGH Open. 2020. PMID: 33102750 Free PMC article.
-
Mucosal imaging in colon polyps: New advances and what the future may hold.World J Gastroenterol. 2022 Dec 21;28(47):6632-6661. doi: 10.3748/wjg.v28.i47.6632. World J Gastroenterol. 2022. PMID: 36620337 Free PMC article. Review.
-
Endoscopic Submucosal Dissection, Endoscopic Mucosal Resection, and Transanal Minimally Invasive Surgery for the Management of Rectal and Anorectal Lesions: A Narrative Review.J Clin Med. 2023 Jul 19;12(14):4777. doi: 10.3390/jcm12144777. J Clin Med. 2023. PMID: 37510892 Free PMC article. Review.
References
-
- Bond JH. Polyp guideline: diagnosis, treatment, and surveillance for patients with colorectal polyps. Practice Parameters Committee of the American College of Gastroenterology. Am J Gastroenterol. 2000;95:3053–3063. - PubMed
-
- Rastogi A, Rao DS, Gupta N, Grisolano SW, Buckles DC, Sidorenko E, Bonino J, Matsuda T, Dekker E, Kaltenbach T, et al. Impact of a computer-based teaching module on characterization of diminutive colon polyps by using narrow-band imaging by non-experts in academic and community practice: a video-based study. Gastrointest Endosc. 2014;79:390–398. - PubMed
-
- Hewett DG, Kaltenbach T, Sano Y, Tanaka S, Saunders BP, Ponchon T, Soetikno R, Rex DK. Validation of a simple classification system for endoscopic diagnosis of small colorectal polyps using narrow-band imaging. Gastroenterology. 2012;143:599–607.e1. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
