

The importance of clinical pharmacokinetic-pharmacodynamic studies in unraveling the determinants of early and late tuberculosis outcomes
- PMID: 30283633
- PMCID: PMC6161803
- DOI: 10.4155/ipk-2017-0004
The importance of clinical pharmacokinetic-pharmacodynamic studies in unraveling the determinants of early and late tuberculosis outcomes
Abstract
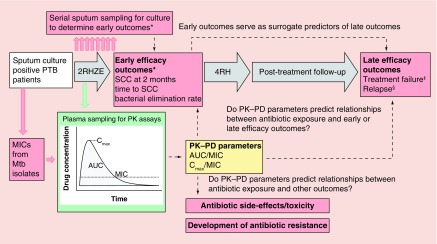
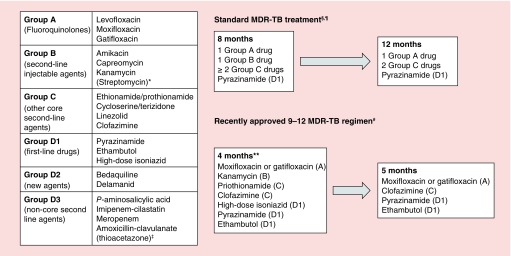
Tuberculosis remains a major infectious cause of morbidity and mortality worldwide. Current antibiotic regimens, constructed prior to the development of modern pharmacokinetic-pharmacodynamic (PK-PD) tools, are based on incomplete understanding of exposure-response relationships in drug susceptible and multidrug resistant tuberculosis. Preclinical and population PK data suggest that clinical PK-PD studies may enable therapeutic drug monitoring for some agents and revised dosing for others. Future clinical PK-PD challenges include: incorporation of PK methods to assay free concentrations for all active metabolites; selection of appropriate early outcome measures which reflect therapeutic response; elucidation of genetic contributors to interindividual PK variability; conduct of targeted studies on special populations (including children); and measurement of PK-PD parameters at the site of disease.
Keywords: clinical trials; compartmental pharmacokinetics; multidrug-resistant tuberculosis; pharmacogenetics; pharmacokinetics–pharmacodynamics; therapeutic drug monitoring; tuberculosis.
Conflict of interest statement
Financial & competing interests disclosure Wellcome Trust (Clinical PhD Fellowship awarded to A McCallum). Grant Number: 105392/B/14/Z. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.
Figures
References
-
- World Health Organization. Global Tuberculosis Report 2016. www.who.int/tb/publications/global_report/en/
-
- Fox W, Ellard GA, Mitchison DA. Studies on the treatment of tuberculosis undertaken by the British Medical Research Council tuberculosis units, 1946–1986, with relevant subsequent publications. Int. J. Tuberc. Lung Dis. 1999;3(10 Suppl. 2):S231–S279. - PubMed
-
- Raviglione MC, Harries AD, Msiska R, Wilkinson D, Nunn P. Tuberculosis and HIV: current status in Africa. AIDS. 1997;11(Suppl. B):S115–S123. - PubMed
-
- Semvua HH, Kibiki GS, Kisanga ER, Boeree MJ, Burger DM, Aarnoutse R. Pharmacological interactions between rifampicin and antiretroviral drugs: challenges and research priorities for resource-limited settings. Ther. Drug Monit. 2015;37(1):22–32. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources