

Development of metastatic brain disease involves progression through lung metastases in EGFR mutated non-small cell lung cancer
- PMID: 30283700
- PMCID: PMC6166474
Development of metastatic brain disease involves progression through lung metastases in EGFR mutated non-small cell lung cancer
Abstract
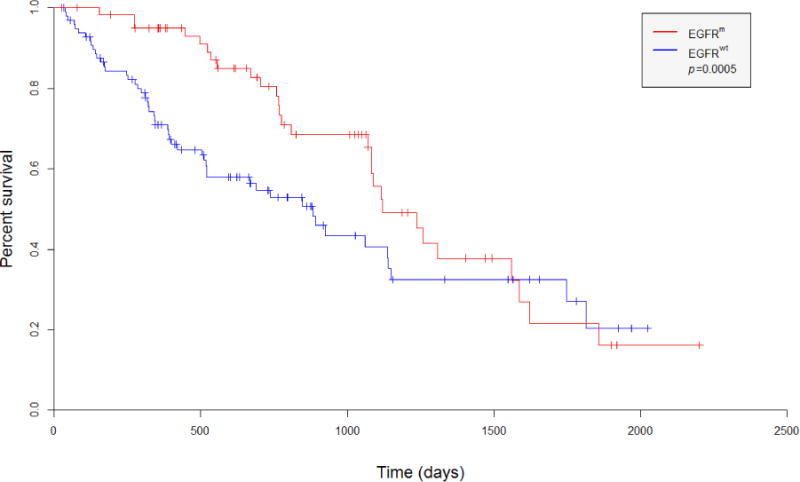
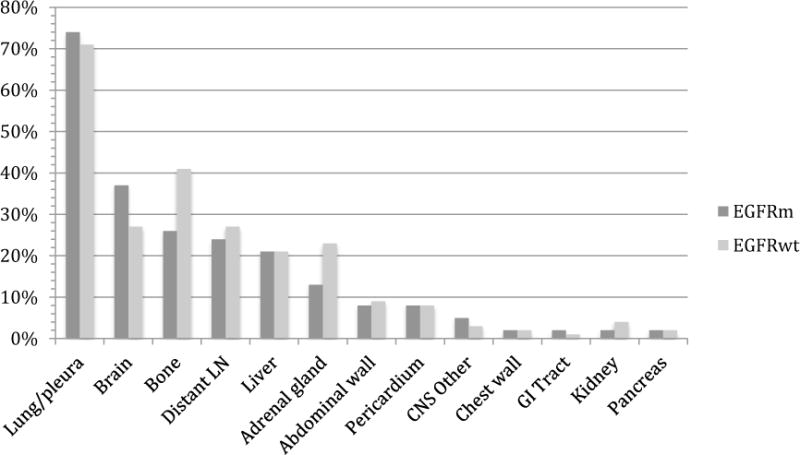
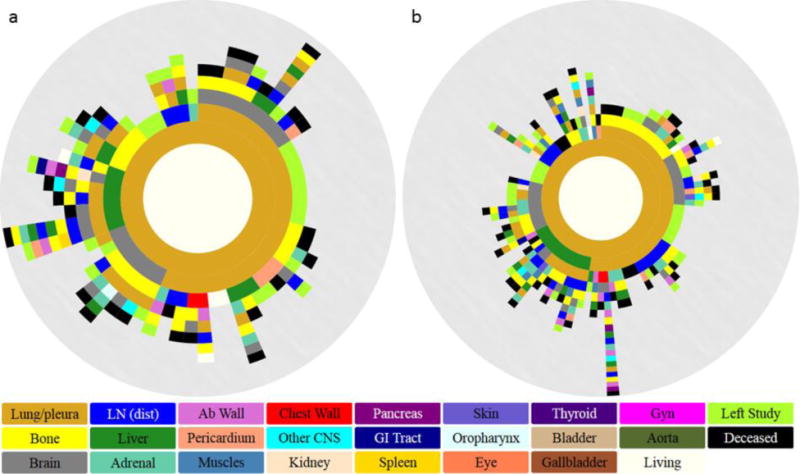
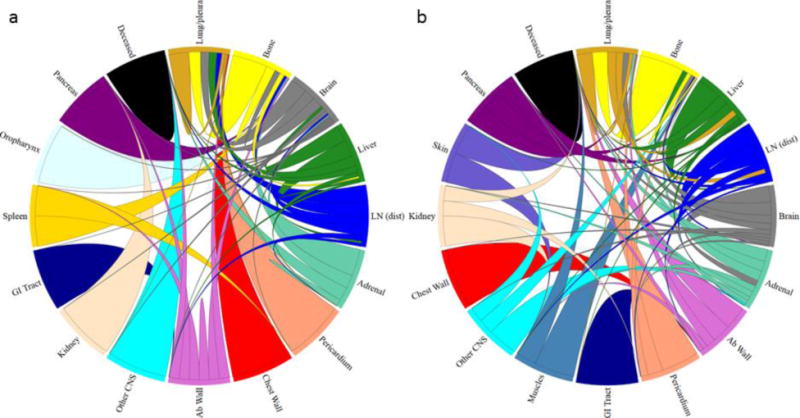
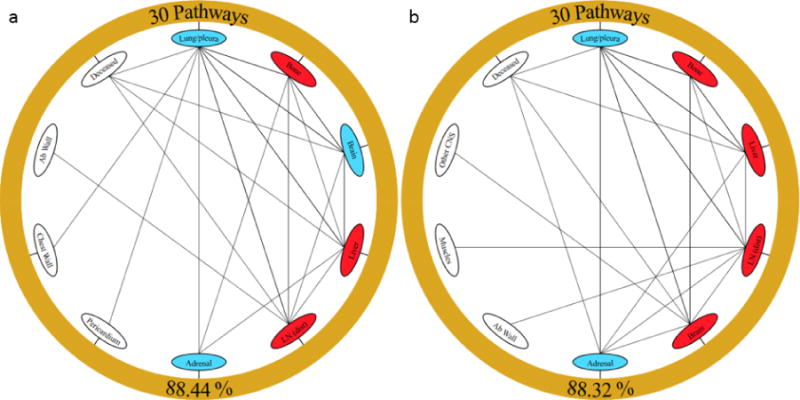
Lung cancer is often classified by the presence of oncogenic drivers, such as epidermal growth factor receptor (EGFR), rather than patterns of anatomical distribution. While metastatic spread may seem a random and unpredictable process, we explored the possibility of using its quantifiable nature as a measure of describing and comparing different subsets of disease. We constructed a database of 664 non-small cell lung cancer (NSCLC) patients treated at the University of Southern California Norris Comprehensive Cancer Center and the Los Angeles County Medical Center. Markov mathematical modeling was employed to assess metastatic sites in a spatiotemporal manner through every time point in progression of disease. Our findings identified a preferential pattern of primary lung disease progressing through lung metastases to the brain amongst EGFR mutated (EGFR m) NSCLC patients, with exon 19 deletions or exon 21 L858R mutations, as compared to EGFR wild type (EGFR wt). The brain was classified as an anatomic "sponge", with a higher ratio of incoming to outgoing spread, for EGFR m NSCLC. Bone metastases were more commonly identified in EGFR wt patients. Our study supports a link between the anatomical and molecular characterization of lung metastatic cancer. Improved understanding of the differential biology that drives discordant patterns of anatomic spread, based on genotype specific profiling, has the potential to improve personalized oncologic care.
Conflict of interest statement
Disclosures: Otherwise, the listed authors have no other affiliations or involvement with any financial or non-financial interests to report.
Figures
References
-
- Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361(10):947–957. - PubMed
-
- Shaw AT, Kim DW, Nakagawa K, et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N Engl J Med. 2013;368(25):2385–2394. - PubMed
-
- Enomoto Y, Takada K, Hagiwara E, Kojima E. Distinct features of distant metastasis and lymph node stage in lung adenocarcinoma patients with epidermal growth factor receptor gene mutations. Respir Investig. 2013;51(3):153–157. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous