

2018 European Thyroid Association Guideline for the Management of Graves' Hyperthyroidism
- PMID: 30283735
- PMCID: PMC6140607
- DOI: 10.1159/000490384
2018 European Thyroid Association Guideline for the Management of Graves' Hyperthyroidism
Abstract
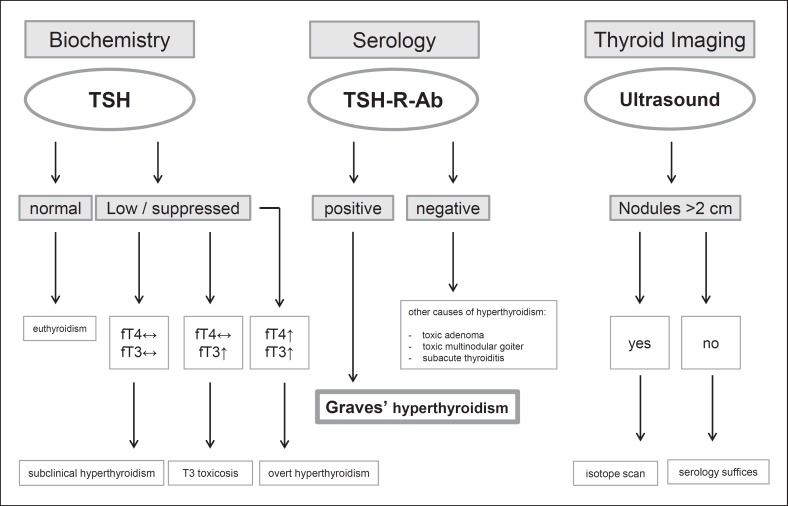
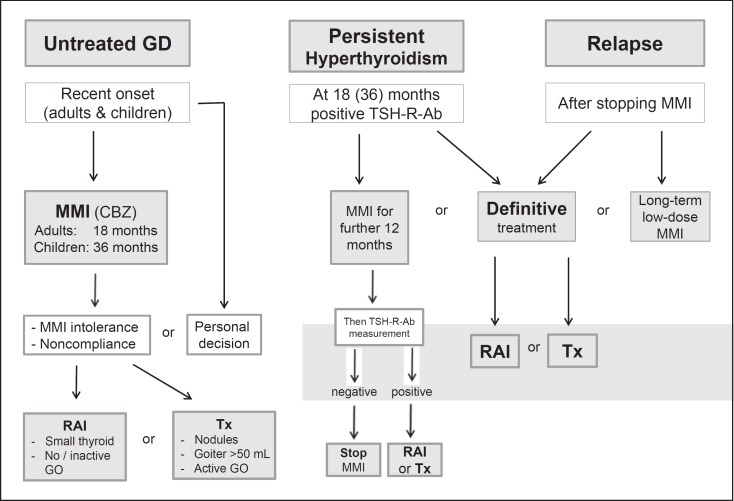
Graves' disease (GD) is a systemic autoimmune disorder characterized by the infiltration of thyroid antigen-specific T cells into thyroid-stimulating hormone receptor (TSH-R)-expressing tissues. Stimulatory autoantibodies (Ab) in GD activate the TSH-R leading to thyroid hyperplasia and unregulated thyroid hormone production and secretion. Diagnosis of GD is straightforward in a patient with biochemically confirmed thyrotoxicosis, positive TSH-R-Ab, a hypervascular and hypoechoic thyroid gland (ultrasound), and associated orbitopathy. In GD, measurement of TSH-R-Ab is recommended for an accurate diagnosis/differential diagnosis, prior to stopping antithyroid drug (ATD) treatment and during pregnancy. Graves' hyperthyroidism is treated by decreasing thyroid hormone synthesis with the use of ATD, or by reducing the amount of thyroid tissue with radioactive iodine (RAI) treatment or total thyroidectomy. Patients with newly diagnosed Graves' hyperthyroidism are usually medically treated for 12-18 months with methimazole (MMI) as the preferred drug. In children with GD, a 24- to 36-month course of MMI is recommended. Patients with persistently high TSH-R-Ab at 12-18 months can continue MMI treatment, repeating the TSH-R-Ab measurement after an additional 12 months, or opt for therapy with RAI or thyroidectomy. Women treated with MMI should be switched to propylthiouracil when planning pregnancy and during the first trimester of pregnancy. If a patient relapses after completing a course of ATD, definitive treatment is recommended; however, continued long-term low-dose MMI can be considered. Thyroidectomy should be performed by an experienced high-volume thyroid surgeon. RAI is contraindicated in Graves' patients with active/severe orbitopathy, and steroid prophylaxis is warranted in Graves' patients with mild/active orbitopathy receiving RAI.
Keywords: Antithyroid drugs; Graves' hyperthyroidism; Graves' orbitopathy; Management; Radioiodine therapy; Thyroidectomy.
Figures
References
-
- Bahn RS, Burch HB, Cooper DS, Garber JR, Greenlee MC, Klein I, Laurberg P, McDougall IR, Montori VM, Rivkees SA, Ross DS, Sosa JA, Stan MN, American Thyroid Association; American Association of Clinical Endocrinologists Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Endocr Pract. 2011;17:456–36. - PubMed
-
- Bartalena L. Diagnosis and management of Graves disease: a global overview. Nat Rev Endocrinol. 2013;9:724–36. - PubMed
-
- Kahaly GJ, Dillmann WH. Thyroid hormone action in the heart. Endocr Rev. 2005;26:704–36. - PubMed
-
- Biondi B, Kahaly GJ. Cardiovascular involvement in patients with different causes of hyperthyroidism. Nat Rev Endocrinol. 2010;6:431–36. - PubMed
-
- Ross DS, Burch HB, Cooper DS, Greenlee MC, Laurberg P, Maia AL, Rivkees SA, Samuels M, Sosa JA, Stan MN, Walter MA. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26:1343–36. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
