

Genetic landscape of pediatric movement disorders and management implications
- PMID: 30283815
- PMCID: PMC6167181
- DOI: 10.1212/NXG.0000000000000265
Genetic landscape of pediatric movement disorders and management implications
Abstract
Objective: To identify underlying genetic causes in patients with pediatric movement disorders by genetic investigations.
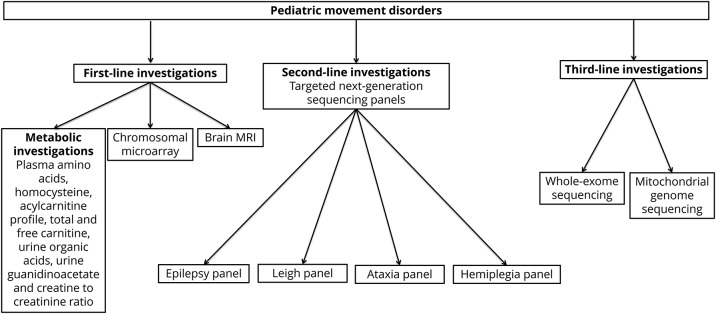
Methods: All patients with a movement disorder seen in a single Pediatric Genetic Movement Disorder Clinic were included in this retrospective cohort study. We reviewed electronic patient charts for clinical, neuroimaging, biochemical, and molecular genetic features. DNA samples were used for targeted direct sequencing, targeted next-generation sequencing, or whole exome sequencing.
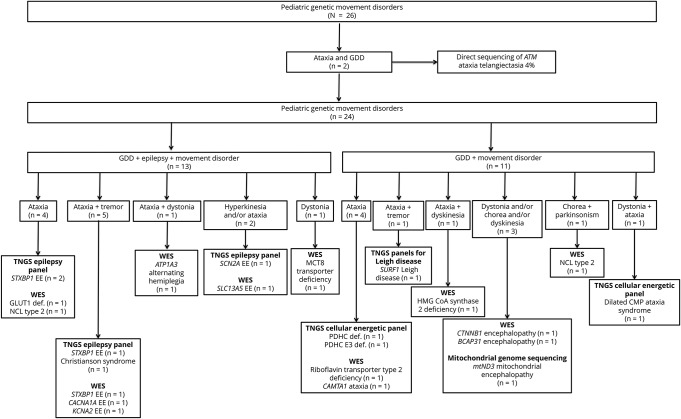
Results: There were 51 patients in the Pediatric Genetic Movement Disorder Clinic. Twenty-five patients had dystonia, 27 patients had ataxia, 7 patients had chorea-athetosis, 8 patients had tremor, and 7 patients had hyperkinetic movements. A genetic diagnosis was confirmed in 26 patients, including in 20 patients with ataxia and 6 patients with dystonia. Targeted next-generation sequencing panels confirmed a genetic diagnosis in 9 patients, and whole exome sequencing identified a genetic diagnosis in 14 patients.
Conclusions: We report a genetic diagnosis in 26 (51%) patients with pediatric movement disorders seen in a single Pediatric Genetic Movement Disorder Clinic. A genetic diagnosis provided either disease-specific treatment or effected management in 10 patients with a genetic diagnosis, highlighting the importance of early and specific diagnosis.
Figures
References
-
- Garcia-Cazorla A, Duarte ST. Parkinsonism and inborn errors of metabolism. J Inherit Metab Dis 2014;37:627–642. - PubMed
-
- Kurian MA, Dale RC. Movement disorders presenting in childhood. Continuum (Minneap Minn) 2016;22:1159–1185. - PubMed
-
- Koy A, Lin JP, Sanger TD, Marks WA, Mink JW, Timmermann L. Advances in management of movement disorders in children. Lancet Neurol 2016;15:719–735. - PubMed
-
- Lumsden DE, Kaminska M, Ashkan K, Selway R, Lin JP. Deep brain stimulation for childhood dystonia: is “where” as important as in “whom”? Eur J Paediatr Neurol 2017;21:176–184. - PubMed
LinkOut - more resources
Full Text Sources